Abstract
This Advance Work Based project presents a case study of how might Service Design Thinking improve service provider and patient experience at a Thalassemia centre and recommendations on how the Thalassemia Centre could continue to use the tools and methodologies introduced to continue to improve the service offered.
This project includes a view on current design thinking, and how service design was used in particular to tackle the task. A few case studies have been explored to get a deeper understanding of how tools and methodologies were used.
Further more, this project shows in depth of how the tools and methodologies were used in the context of a Thalassemia centre. Qualitative research methods where adopted through shadowing, contextual interviews, focus groups, journey maps, mobile ethnography and many more.. Prototypes were also made in order to visualize how the service could be improved. The process was co creative where several stakeholders of the service were involved in the design process.
Finally an implementation plan was put into place and recommendations on how the service provider could continue to adopt the tools used.
Keywords: Design thinking, Service Design, Human Centered Design, Prototype, Thalassemia, Co creative.
Preface/Introduction
Preface
My journey began when I decided to join Hyper Islands Masters Digital Media Management program. I had previously been a multidisciplinary designer practising Interaction, Motion and Communication design. I had studied and worked in Canada for about 4 years and I felt that I needed to go back to my own country and provide the valuable knowledge I had learnt in the west. I mostly worked on my own as a free lancer and did not have much experience working with teams. I also knew that going back to Pakistan as a basic designer would not generate that much income for me. My goal was to have my own design agency in Pakistan. In order to do that I had to enhance my skills of team building, leadership and managing projects. Hyper Islands DMM program was a perfect fit, as it covered those areas of expertise plus a lot more.
At Hyper I was introduced to Design Thinking, Digital Technologies, Business Transformation and the Start up Module. During the Design Thinking module Andy Young who was our mentor introduced us to Service Design. He was working for Snook a service design agency. I had been familiar with User Experience design in the past but had no idea that there was a process for designing services. I was always curious to know how it worked.
I was then contacted by Maria and Katie to create a brand identity for their company. Their company is called Amity, which happens to be a social enterprise working with a human-centered approach. (amity,2014). Working with them made me learn more about service design and how it can lead to social impact.
In our last module Start up, me and four other team mates collaborated together to start a Service Design agency. Our goal was to make a strong brand and to see if we were hirable. Turned out that we worked on two briefs out of which one of them wanted to take the project forward towards implementation. Unfortunately our time at Hyper was over in Manchester and each one of us had to go our separate ways and work on our Advance work based project.
My love for service design continued. For my advance work based project I wanted to understand how service design was practiced in the west and bridge it with how it is being practiced in Pakistan. To my surprise when I came back to Pakistan and started exploring who was practicing service design thinking, it turned out that there was no agency. In this case I had to shift my focus and I thought to my self then why don’t I introduce service design thinking to Pakistan. My supervisor told me that was to broad and I needed to narrow my focus.
I was fortunate enough to be the Brand Manager at Husain Blood Bank in Pakistan. I knew that they were offering a service. I requested the management if I could do a pilot project with them to see if service design thinking could have an impact on creating value for their customers and the organization as well. As soon as I began my research I realized that customers at the blood bank would only come in times of an emergency and that regular donors, only could donate a maximum of four times a year (Wales, 2014). So in order for me to conduct the project with these samples I would have to work for at least a year to gather data. I did not have such luxury with time as my thesis had a deadline. The management then suggested that I could work with their Thalassemia Centre, and could possibly get better results there. This was because Thalassemia major patients would visit the center every 2-4 weeks as they required transfusions depending on the individual’s consumption of infused cells.(Thalassemia.ca, 2014). This worked out in my favour as it allowed me to test the tools and methods, receive feedback and possibly see the impact of my work in the provided time allotted for my advance work based project.
I would like to thank, Husaini Hematology and Oncology Trust, for allowing me to do to this project, my supervisors Jakob and Jerel for guiding me through out the project and finally the Staff and Patients at the center without whom I would have not been able to get such great insights and feedback on the process.
Introduction
“Intentionally or unintentionally, design and its process have formed and styled the world we live in. Design surrounds everyday life to such an extent that designers and their processes have become largely invisible, vastly misunderstood and subsequently undervalued by society. Service design is playing an important role in shifting these perceptions, by breaking down preconceived notions of creativity, actively illustrating the significant and wider social application of design, involving more people in the design process.”-Kate Andrews (Stickdorn and Schneider, 2011)
“Working with experience is to service design what working with communications is to graphic design.” Service design works when we provide positive experiences to people – clients, users and consumers – by making sure that it meets or goes beyond their expectations. Experience is important because it allows people to tell stories about how they use and are affected by services. This creates opportunities for innovation and improvement as well as provides an opportunity to visual future experiences.(Polaine, Løvlie and Reason, 2013)
In this advanced work-based project, I researched how service design thinking could improve service provider and patients’ experiences at Husaini Thalassemia Centre(HTC) in Pakistan and recommendations in ways in which the centre could continue to utilize the tools and methods introduced to further improve their current and future services. First, I will explore what design thinking is and the different types of experiential design. I will then draw information from several case studies relating to how service design thinking is applied in context to other services including healthcare. I will take you through my entire journey from the research tools and methods used, prototypes created to an implementation plan and suggestions on how the service can continue to innovate and create new experiences.
Husaini Thalassemia Center is a subsidiary of Husaini Hematology & Oncology Trust (HHOT) a not for profit NGO where 411 thalassaemia major registered patients are receiving 100% free of cost supporting treatment like doctors consultation, blood & its components, iron chelating drugs, general medicine, surgical procedures, food, fare, recreation tours, etc.
Design Thinking
“The term “design” is commonly associated with products’ quality and/or aesthetic appearance, the main goal of design as a discipline is to promote well being in people’s lives. Nonetheless, it is the way that designers perceive things and act upon them that has attracted the attention of management, opening new paths to business innovation.” –Vianna, M., Vianna, Y., Adler, I., Lucena, B. and Russo, B. A designer’s main task is to identify a problem which disrupts the human experience and create a solution for this disruption. (Vianna et al., 2012)
“Design is a process where we create and shape artifacts that solve problems”- Peter J. Denning (Denning, 2013)
I believe that design is the gaining of insight into a client’s or user’s needs and problems and coming up with a creative solution for them.
“Design thinking has come to be defined as combining empathy for the context of a problem, creativity in the generation of insights and solutions, and rationality in analyzing and fitting various solutions to the problem context.” – Tom Kelly Dave Kelly (Kelley and Kelley, 2013)
Tim Brown says that the goal of design thinking is “matching people’s needs with what is technologically feasible and viable as a business strategy.” -Tim Brown (Brown, 2014)
During a TED Talk, Tim Brown suggested that design is getting big again and it is happening through the applications of design thinking to new problems such as global warming, education, health care, security and clean water. He also mentions that design thinking is a new way of tackling problems. Before this, we would take a convergent approach where we made choices based on our available alternatives whereas if we now take a divergent approach, it allows us to explore new alternatives, new solutions and new ideas that may have not existed before. (Brown, 2009)
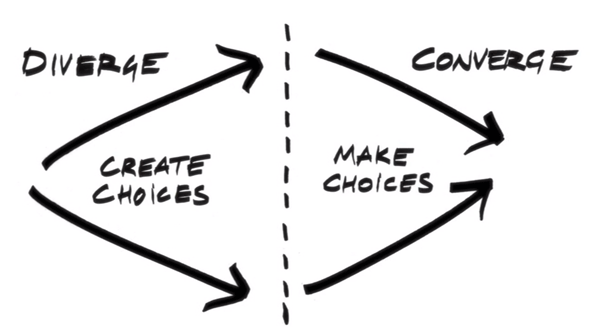
(Brown, 2009)
“Moreover, as the name itself conveys, Design Thinking refers to how the designer thinks, drawing on a style of reasoning that is hardly conventional in the business world, known as abductive thinking. Abductive thinking endeavors to formulate inquiries through the apprehension or comprehension of phenomena, that is to say, questions are posed to be answered using information gathered from observation of the context pervading the problem. In abductive reasoning, therefore, the solution does not derive from the problem: it patterns itself after the problem.
One cannot solve problems with the same kind of reasoning that created them: abducting and defying the conventions of business is the foundation of Design Thinking. It is by reasoning abductively that designers constantly challenge their standards, making and unmaking conjectures and transforming them into opportunities for innovation.” –Vianna, M., Vianna, Y., Adler, I., Lucena, B. and Russo, B (Vianna et al., 2012)
There are a few processes to design thinking:
According to Simon Herbert they are: define, research, ideate, prototype, choose, implement and learn. (Warner and Simon, 1969)
According to Daylight (a design agency) the process is: learn from people, look for patterns, define the design principles, make tangible and iterate relentlessly.
Daylight says “design thinking is a powerful tool to reveal new ways of thinking and doing”-Daylight (Daylight, 2014)
A case where design thinking was used was at Kaiser Permanente, a healthcare provider in the U.S. The project was run by Innovation Consultancy (IC), a team of creative people within Kaiser Permanente focused on developing and implementing evidence-based and human-centered innovations at the frontlines of healthcare delivery.(Zuber, 2011)
The IC process:

(Zuber, 2011)
They wanted to improve patient experience, and focused on how knowledge was exchanged during shift changes. They used observational research, shadowing, video ethnography, brainstorming new solutions and rapid prototyping. They came up with NKEplus, a system that enables nurses to be at the bedside for shift changes.(Kaiser Permanente, 2012)This brought the time the nurses were away from patients from 40 minutes down to 12 minutes on average. This increased patient confidence and nurse happiness. (Tim brown’s TED Talk).
This case study made me realise that wait time was something I could explore for my project.
Service Design
There are several definitions, methods, tools and processes to service design. I would like to explore a few of them. I primarily used these two books This is Service Design Thinking and Service Design: From Insight to Implementation as my sources for gaining knowledge on this topic. I also took inspiration from service design agencies and articles from the Teeside University database.
“Service Design helps to innovate (create new) or improve (existing) services to make them more useful, usable, desirable for clients and efficient as well as effective for organisations.
It is a new holistic, multi-disciplinary, integrative field.” — Stefan Moritz, 2005 (Stickdorn and Schneider, 2011)
“Service Design is an emerging field focused on the creation of well thought through experiences using a combination of intangible and tangible mediums. It provides numerous benefits to the end user experience when applied to sectors such as retail, banking, transportation, and healthcare.
Service design as a practice generally results in the design of systems and processes aimed at providing a holistic service to the user.
This cross-disciplinary practice combines numerous skills in design, management and process engineering. Services have existed and have been organized in various forms since time immemorial. However, consciously designed services that incorporate new business models are empathetic to user needs and attempt to create new socio-economic value in society. Service design is essential in a knowledge driven economy.”
— The Copenhagen Institute of Interaction Design, 2008 (Stickdorn and Schneider, 2011)
“Service design is a design specialism that helps develop and deliver great services. Service design projects improve factors like ease of use, satisfaction, loyalty and efficiency right across areas such as environments, communications and products – and not forgetting the people who deliver the service.”
Engine service design, 2010 (Stickdorn and Schneider, 2011)
Principles of Service Design
Marc Stickdron states the five principals of service design are:
1. User-Centered: This is where the service should be experienced through the customer’s eyes
2. Co-Creative: All stakeholders should be included in the service design process
3. Sequencing: The service should be visualized as a sequence of interrelated actions.
4. Evidencing: Intangible services should be visualized in terms of physical artifacts
5. Holistic: The entire environment of a service should be considered.
(Stickdorn and Schneider, 2011)
I will dig deeper into each of these principals as well as examine at other service design approaches.
User-Centered
One needs to put the customer or the user at the center of the design process. To better understand the service we need to see it from the customer’s perspective. This allows us to gain insights on the experiences the customer or the service provider is having with the service.
IDEO looks at this principle as “human-centered.” They use this term because the design process starts with the people we are designing for. It examines the needs, dreams and behaviors of people that are affected by solutions created or proposed. I will further investigate this process in another section.(IDEO, 2011)
When thinking about user-centered, it is important to consider certain factors such as the physical differences of users, their motivations, expectations, previous experiences, the type of activities carried out and where the activities are carried out. If these are not taken into account, it can lead to negative experiences that promote frustration, accidents, injuries, cumulative stress and waste time or money.
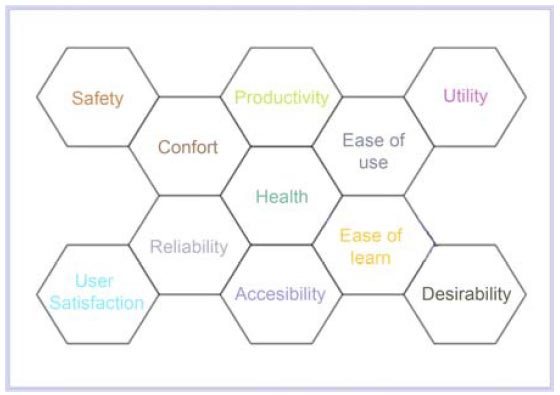
The figure above helps designers set goals to identify problems that users may have to speed up decision making during the design process. (Alejandro and Colin, 2012)
Co-Creative
There are many stakeholders involved in a service and each one has different needs and expectations. Each individual brings different perspectives and ideas to the table. This allows one to build on each other’s ideas. Allowing the customer to be involved in the process allows the service provider to be more likely to satisfy their needs. This also gives a sense of co-ownership which increases customer loyalty and long-term engagement. (Stickdorn and Schneider, 2011)
Services only have value when a customer uses them. It is a missed opportunity when some organizations don’t think about their customers as valuable, productive assets in the delivery of a service, but just as anonymous consumers of the product or service. (Polaine, Løvlie and Reason, 2013)
The customer is always a creator of value: there is no value until and unless the offer is used; experiences and perceptions are essential to value determination. –Steve Vargo, Robert F Lusch (Steve Vargo. and Lusch, 2012)
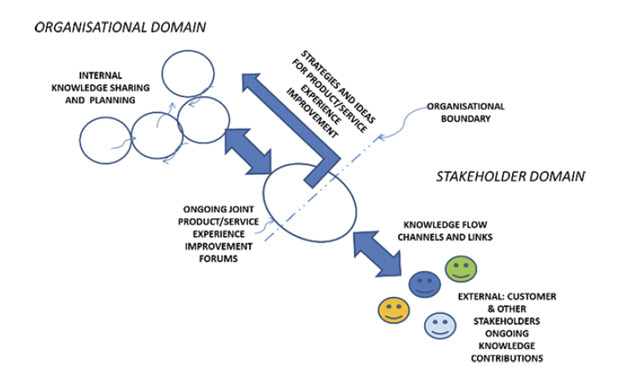
The figure above demonstrates key components of a co-design process. It shows knowledge sharing between customers and the organization in finding strategies to improve customer experience. (Perrott, 2013)
Sequencing
If we look at a movie it is a series of static pictures. The same way service design thinking looks at this analogy to deconstruct a service into a series of single touch points or interactions the user is engaging in. When they are combined, they create service moments. Each service process follows a three step transition of pre-service, the actual service and the post service. (Stickdorn and Schneider, 2011)
“Service quality can be defined by how well the touch points of the service work together for the customer.” All these interactions together make up the service experience.–Andy Polaine, Lavrans Løvlie and Ben Reason
Evidencing
A service is usually only acknowledged when the user experiences it. However, some services are invisible and the customer and service provider take them for granted. Services such as electricity and water are a good example of this. It is only when the service is cut off that the user may recognize its absence. This is why it is very important for a service designer to make the invisible visible by showing the customer what is going on behind the scenes and showing the staff what the customer is feeling. (Polaine, Løvlie and Reason, 2013)
This was very important in the creation of the physical token prototype at the Husaini Thalassemia Centre to illustrate the experience of both the user and the service provider.
Holistic
It is important for all the touch points to come together in order to see the larger picture. Keeping all stakeholders in mind and the multiple journeys they go on together makes up the entire experience of the service. One also needs to see the organizational structure, process, values and culture of the service provider. This helps set the mindset of the customers as well as the employees. (Stickdorn and Schneider, 2011)
The next section will explore a couple of case studies of how service design is used practically.
Case Studies of Service Design
Tailoring services for Virgin’s customers (Engine Group, 2013)
Client: Virgin Atlantic Airways (VAA)
Agency: Engine Group
The challenge for VAA was to redesign and expand their presence in London’s Heathrow Airport Terminal 3. They then engaged Engine Group in a collaborative process between VAA’s in-house service design team and Engine in visualizing the future experiences of their customers for each class.
Engine approached it from the customer’s perspective but also involved other stakeholders such as the terminal staff, and the service providers. A customer journey map was delivered with detailed specifications of several touch points.
They used tools such as shadowing, contextual interviews, journey mapping and service blue prints. They improved the flow of the process and designed a unique experience for first class where they would have a Drive Through check in facility, porter service, pre-emptive baggage-weigh, a lounge area and an exclusive Virgin security lane. They analyzed each touchpoint and created an implementation plan of the benefits for each concept through customer experience scenarios.
The results led to a 75% reduction in check-in times, and an increase in Customer Service Index (CSI) by 30%. The Upper Class wing and Economy Class provided high ratings for each touchpoint.
From this case study, I learnt that it is important to map out the flows and journeys of both the customer and service provider. It is also important to have a collaboration between the client and agency. It was very insightful to learn about an organization such as VAA which had its own internal service design team. Finally, reduced wait times and better experiences at each touch point would be something to look into for my project.
Embedding community engagement (Engine Group, 2011)
Client: Buckinghamshire County Council (Bucks)
Agency: Engine Group.
The challenge was “In 2008, local authorities were being encouraged to embed a culture of engagement and community empowerment when developing services, with the view to achieve real service improvement and more economical delivery.”
Engine was asked to help the council realize this approach through a practical project and allow them to learn new skills and approaches to community engagement, keeping in mind improving health and social care for residents over 50.
The result was HealthConnect, “a service development proposal designed to improve access to health and social care services in Buckinghamshire. “
This was a co-design approach. Engine used a methodology known as SHAPE, “Services Having All People Engaged,” which they produced themselves for people-centered services. Input from the residents was essential to the development of the service. Engine researched opportunities and problems of day-to-day activities of the elderly in the community, and used the insights to help elect members residents, officers and service providers.
HealthConnect included channels of how users could get useful information, and how transport providers could work collaboratively together to help residents access their services.
The SHAPE methodology had an impact on several organizations, who then integrated it into their own organizations.
From this study I learnt that co-design is very important to the development of services. I also learnt that age is not a limitation when being part of a design process. Lastly I learnt that each project has a different approach and that new tools and methodologies can come out from a project. (You can see how I managed to evolve the Card Sorting tool)
Design for the clinic Experience
(Cliver et al., 2007)
(Stickdorn and Schneider, 2011)
Client: University of Pittsburgh Medical Centre (UPMC)
Team: Carnegie Mellon School of Design
The challenge for the team was to improve wait time, work flow for staff and way finding. Their insight was that patients needed more information, support and engagement. They proposed a holistic solution; they said that the concepts they presented could be implemented individually but put together would be part of a whole. Since the solutions were involving all stakeholders (patients, families, staff and physicians) excluding any one of these groups would not provide a holistic solution.
Their proposals included: Wall of Hope, Welcome Booklet, Clinic Chat, Gift from the Clinic, Clinic Staff Locator, Clinic Staff Meetings, Wait time indicator and PCP Direct Link. Wall of Hope provided a space where patients wrote testimonials about the doctor, engaging the patients while they waited whether they read the notes or wrote one themselves. Welcome Booklet was a handout for patients to get information and a line of interaction between the staff and the user. Clinic Chat, an organically formed system, would allos interaction with the staff members not available. Gift from the Clinic, was a token of appreciation and positive interaction between the patients and staff members. Clinic Staff Locator was a tracking device using RFID that allows nurses to locate doctors and vice versa. Clinic Staff Meetings would be helpful for team building and professional development. Wait time indicator was a display that would provide information on how much time was spent with and away from patients. PCP Direct link was an interactive display that would allow the doctor to consult with other physicians or staff members.
The team used several tools such as territory mapping to visualize the space, observations and interviews to gather deeper insights, service blue prints, participatory design activities, experience cards to imagine alternate clinic experiences, what if scenarios, patient journeys, sketching concepts, storyboards to validate ideas and example interfaces (prototypes).
The concepts were presented to the Center for Quality Improvement and Innovation and other UPMC staff, and they loved them. Unfortunately, these concepts were never implemented. Their greatest success was the ability to empower the staff to believe that they could make small changes themselves to improve patient experience. The team also learnt that even though the project was not implemented, the process of applying service design thinking was invaluable. They appreciated the difference between designing for products versus designing for services.
I learnt a lot from this case study as I was going to perform my project at a thalassemia center. There are many similar stake holders like the case above. I learnt that a holistic approach is key to creating a better experience both for the patient and service provider. I learnt that more than one concept can be presented based on different insights. The team used several tools and I would like to do the same to see different results. As I am a student, I fear that I may not be taken seriously and my concepts may also not be implemented.
Looking at other approaches.
Human Centered Design
During my time at Hyper Island, I was introduced to Human Centered Design (HCD) through a course with +Acumen partnering with IDEO. (+Acumen, 2014)
The course was a series of workshops and an introduction to the Human Centered Design tool kit. (IDEO, 2011)
My leanings and understandings of Human Centered Design are as follows.
“Human-centered design is innovation inspired by people.” –IDEO
HCD is a process of working with teams to transform difficult challenges into desirable solutions through design. One needs to be intuitive, recognize patterns and come up with ideas which are functional and meaningful beyond words and symbols. It has four characteristics, which are:
Empathetic: The deep understanding of needs and motivations of people.
Collaborative: Working with others, and seeing multiple perspectives.
Optimistic: No matter what the challenges are one needs to believe that anyone can create change.
Experimental: One can not expect to be perfect. HCD is all about experimenting and learning by doing.
Human Centered Design can be used to create and improve, products, spaces, services and systems.
There are three phases to the human-centered design process. Each phase moves between abstract and tangible. These phases include:
Discover: Going out into the field and learning from people.
Ideate: Narrowing down your learnings and translating them into themes and patterns. Coming up with ideas.
Prototype: Making your ideas tangible and iterating based on real feedback.
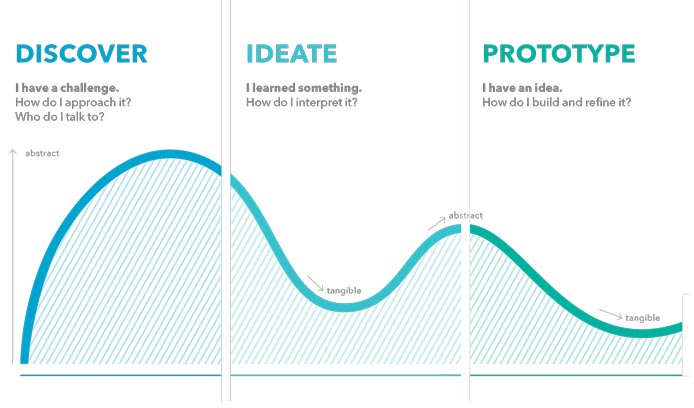
Image from the HCD workshop. (+Acumen, 2014) First 3 phases of HCD.
During the end of the course, in the last workshop, I discovered a phase that was not mentioned in the beginning. It was the phase of:
Moving forward: Testing your ideas and making an implementation plan on how to integrate them with the service.
Case study of how HCD worked.
In Nairobi, Kenya 61 percent of people did not have access to clean drinking water. Many young children were vitamin A deficient, and diarrheal diseases were rated among the top 10 that caused morbidity and mortality.
IDEO partnered with WSUP, GAIN, Aqua for All and Unilever to help improve access to clean water, personal care products, health and education.
Their results were SmartLife, a retail business and brand that offered clean water and health and hygiene products. It is currently running successfully in several places around the city.
The team rented an apartment in order to conduct workshops and an area to build prototypes. They initially conducted a dummy brand and went out in the market to see the response of the service and product they were trying to sell. They learnt that strong branding inspired trust within the community. People were also willing to give a down payment for water delivery for the next day, which was unheard of in Kenya.
As it was a test project, the IDEO team visited the customers and refunded their money letting them know that the business did not exist yet, but it was coming soon. They gave them cans of clean water for their participation in the project.
Once the team returned to San Francisco, they worked on bringing the brand to life, through the creation of business models and understanding logistics. IDEO then presented the design concept, strategies, brands and business models to its partners and SmartLife store opened 6 months later in Nairobi.
(Designkit.org, 2014)
What I learnt from this case study and HCD and how it applies to my project is that it is very important to immerse yourself in the location you are researching. It is important to prototype and come up with ideas at the location of the project. Creating a dummy project was an interesting way to test if the idea would work or not as opposed to investing money in a pilot might not work. It is very important to see if the project is viable and feasible in order for it to be implemented. Having partners helps in the implementation of a project as they bring different skill sets and resources to a project.
Understanding Experience
As my project focuses on improving patient experience, it was important to understand what experience is and the different types of experience in context to service design and my advance work based project.
Experience is “the process or fact of personally observing, encountering or undergoing something.” (Dictionary.com, 2014)
This is my understanding of the four types of experiences mentioned in the book Service design (Polaine, Løvlie and Reason, 2013), which are relevant to service design and my project in particular.
User Experience: The result of users perceptions and responses to task-based activities. As a user completes each task successfully and with ease, it makes a service more successful. “Individuals are generally trying to use tangible elements of a service, such as signage, interfaces, and communications, as they complete everyday tasks.” -Andy Polaine, Lavrans Løvlie and Ben Reason. One needs to understand tasks, timeframes, and interactions and non-human touch points.
Customer Experience: The sum of task-based experiences the user is having with a service. Customer experience is about managing the users’ expectations and delivery of service against what is actually being delivered.
Service Provider Experience: How the experience is delivered from the other side. This is about understanding what is happening behind the scenes to deliver the service. There are times when the service provider is a user as well. For instance a nurse, they provide a service to the patient as well as the doctor and they use the internal services such as interacting with the computers and other equipment.
Human Experience: The emotional effect of the service, and impact on quality of life. When designing for services it is important to understand the impact they have on users’ emotions and senses. If one has a negative human experience, it’s not just about frustration, negative brand image, or a loss in sale but “it affects the development of people’s lives.” –Andy Polaine, Lavrans Løvlie and Ben Reason. Human experience is essential in public services such as health care, transportation and energy as the users often have no alternative. (Polaine, Løvlie and Reason, 2013)
In relation to my advance work based project, it is essential to understand how we are providing these experiences to our thalassemia patients as well as the service provider. The patients may not have an alternative and it is important to give them a positive experience so that it does not have an effect on their emotions or health. My project will touch on how each of these experiences are felt by our stakeholders at different touchpoints within the service.
“Service designers cannot single-handedly change the world, but they can offer a set of methods and approaches to help bridge the gap between service systems and human value” –Andy Polaine, Lavrans Løvlie and Ben Reason (Polaine, Løvlie and Reason, 2013)
Approach
“The first step of a service design process is to design the process itself”. – Marc Stickdorn, Schneider Jakob.
The process described in This is Service Design thinking is an iterative approach. At every stage of the process, one may take step back, reflect and start again from where the team left of or even start over from the beginning. During the process one needs to look at the details of each touchpoint but also keeping in mind the whole customer journey. When working with staff members its important to “understand the organisational structure as a whole” –Marc Stickdorn. During the process one may have to deal with unexpected dilemmas and paradoxes.
The four stages of process are:
- Exploration
- Creation.
- Reflection.
- Implementation.
Exploration: Is the process of discovery, of gaining insights, identifying problems and opportunities. Even though we mainly design for the user, the process may not start there. It is important to first understand the culture are goals of the company providing the service. It is important to educate the service provider about service design and to see if they are willing to come on board the process. The second part is not about finding solutions but immersing yourself in the service to identify real problems. Lastly its taking the findings, creating clusters and identifying themes and problems we want to tackle.
Creation: This stage covers the coming up of ideas, creating prototypes and testing them. At this stage it is very important to keep in mind the Service Design principles as the process needs to be co-creative, keeping in mind each touchpoint and looking at the service as a whole.
Reflection: Once the ideas are tested it is important to get feedback from the users as well as the service providers, in order to iterate and re create scenario. It is important to create prototypes in the real setting of the service as it allows the team to understand the closest result to the end delivery.
Implementation: This final stage is working with the management team to implement the solutions. Before it is implemented it is essential for the concepts to be tested in rigorous detail. Involvement of the staff from the beginning of the process is very important as their motivation and engagement is crucial for a sustainable service implementation. Finally once the changes are implemented it is important to re explore and reevaluate the progress and that in itself becomes an iterative process.
(Stickdorn and Schneider, 2011)
Initially I had spoken with the management about doing this project and they were willing, eager and very excited. I had to then get the rest of the staff members on board. In order to do that I set up a meeting where I presented what service design was and the approach I was going to take towards the project. From the CEO to the Janitor were all present in the board room. This was the first time that the entire team had met together for a meeting and the response was very positive. The staff members felt value and were excited about the project. They were so excited that we had a group discussion right after that, in which they took me through the entire customer journey in brief and started identifying problems on the spot. This process gave the staff members an opportunity to voice their thoughts and opinions. Our journey began here and we continued the process for several weeks to follow.

Introducing the team to the project.

Explaining what service design is. It was a great challenge to present in my native language Urdu, so I had to keep switching between the languages to explain specific processes.
Explaining the Double Diamond as the approach we were going to take for the project.
Double Diamond

The next couple of sections will take you on our journey of how we went through each stage and which tools and methods we used.
Discover: Immersing yourself in the service to find insights, problems and opportunities.
Define: Identifying users needs, creating themes, clustering problems and narrowing in on what aspects of the service you want to focus on.
Develop: Generating ideas, creating prototype and testing them in the space.
Deliver: Presenting concepts, solutions and plans to bring about change.
Tools and Methods
Once I was briefed on how the service was operating, the next step was to decide which tools and methods to use. I decided to mainly use the tools and methods introduced in the book This is Service Design Thinking as it was a collection of many tools introduced by several contributors. I used so tools from the HCD tool kit as well. Each tool was used at relevant stages of the Double Diamond process.
For the project to be successful it needed to be co creative with agile development. Having all stakeholders involved in the iterative process was important as we would be gaining more insights and problem solving minds given the short time frame of the project.
The tools and methods used during the stages included:
Discover/Define
- Stakeholder Maps
- Customer Journey Maps
- Service Blueprints
- Storyboards
- Contextual Interviews
- Shadowing
- Mobile Ethnography
- Storytelling
- A Day in the Life
- Card Sorting
- Expectation Maps
- Service Roleplay
- Service Safari
Develop/Deliver
- Idea Generation
- Service Prototypes
- Service Staging
- Desktop Walkthrough
- What If
- Design Scenarios
- Business Model Canvas
Each tool and method was introduced relevant to the stage of the process we were on. I facilitated the use of the tools and methods. The team then reflected on the process and gave feedback on how it could be improved for future use.
Stakeholder Maps
Stake holder maps allow us to understand our key stakeholders, how they relate to our service.(BSR,2011). It visually or physically represents the the relationships between each member in the service (Stickdorn and Schneider, 2011). It is used to highlight possible issues within groups. It gives us an overview through clusters. It helps identify which group of people play a more significant role than others in the provision of the service.
I started my project with the Thalassemia Center with this tool. I started by talking with the floor manager. He gave me an overview of how the service worked and who all were involved in the process. I then identified the main stake holders in the service and began to interview them. Talking to more people really helped as I identified more key stakeholders in the process whom I was not aware of. Mapping the stakeholders helped me identify who I needed to perform deeper contextual interviews with. A few of the people I spoke with included the Floor Manager, CFO, CEO, Head of Department, Cross Matcher(Lab Technician) and the Office Assistant. The reason I chose these people to speak with was because some of them were more senior level whilst others were on ground operations. This gave a general overview of the interactions between each member. The reason I did this was because it would be very difficult to get in contact with each and every member in time for my project.

The figure above shows the 4th iteration of the stakeholder map.
Key Learnings:
- ● Top level management were only involved if there was a serious issue.
- ● Top level management only spoke with other senior level members who were in charge.
- ● Top level management was not involved in seeing each touchpoint but rather the whole picture.
- ● There had not been any meetings with the trustees in a long time to discuss problems and concerns.
- ● No system set up for meetings.
- ● Limited training for new staff members.
- ● Not all doctors are blood specialists. A platform for skill sharing should be provided.
- ● HR should provide training to staff members before hiring them.
- ● Transport and Ambulance problems. No proper pick and drop service.
- ● Guards are not doing thorough checking
- ● No female guard members.
- ● Patients require more than one bag of negative blood sometimes and it is in limited supply.
- ● Toilets are not cleaned often and the janitors are shouted at.
- ● The janitors sometimes do the runners job
- ● Runners are difficult to find.
- ● Difficulty sending blood between rooms.
- ● Air condition does not work well in the summer time.
- ● No common area for sitting.
“If smaller problems get solved the larger picture can get better” – Lab technician
Limitations: The limitations of this tool are that in order to create a stake holder map it is essential to try to identify each and every member who could have some influence on the service, which may be difficult at times. It takes a significant amount of time as one needs to understand the relationship and interaction between each stake holder and for a very large organization it could be problematic. Even with our project it went through 4 iterations as the more people we spoke with the more stakeholders we identified. It was not possible to speak with all stake holders in the given time.
Customer journey maps
“The customer journey map is an oriented graph that describes the journey of a user by representing the different touchpoints that characterize his interaction with the service.” Roberta Tassi (Tassi, 2009)
It is time based and shows the different channels the user is interacting with. A visual representation of the journey helps create empathetic engagement and helps tell the story of the experience the user is going through. (Stickdorn and Schneider, 2011)
At the Thalassemia Center we mapped this out with the help of the staff members and the patients. We learnt were there was opportunity for improvement within the service. We also realized that it was important to also see the journey of the blood, as it was one of the products which was part of the service. You can see that in the Service Blue Print.
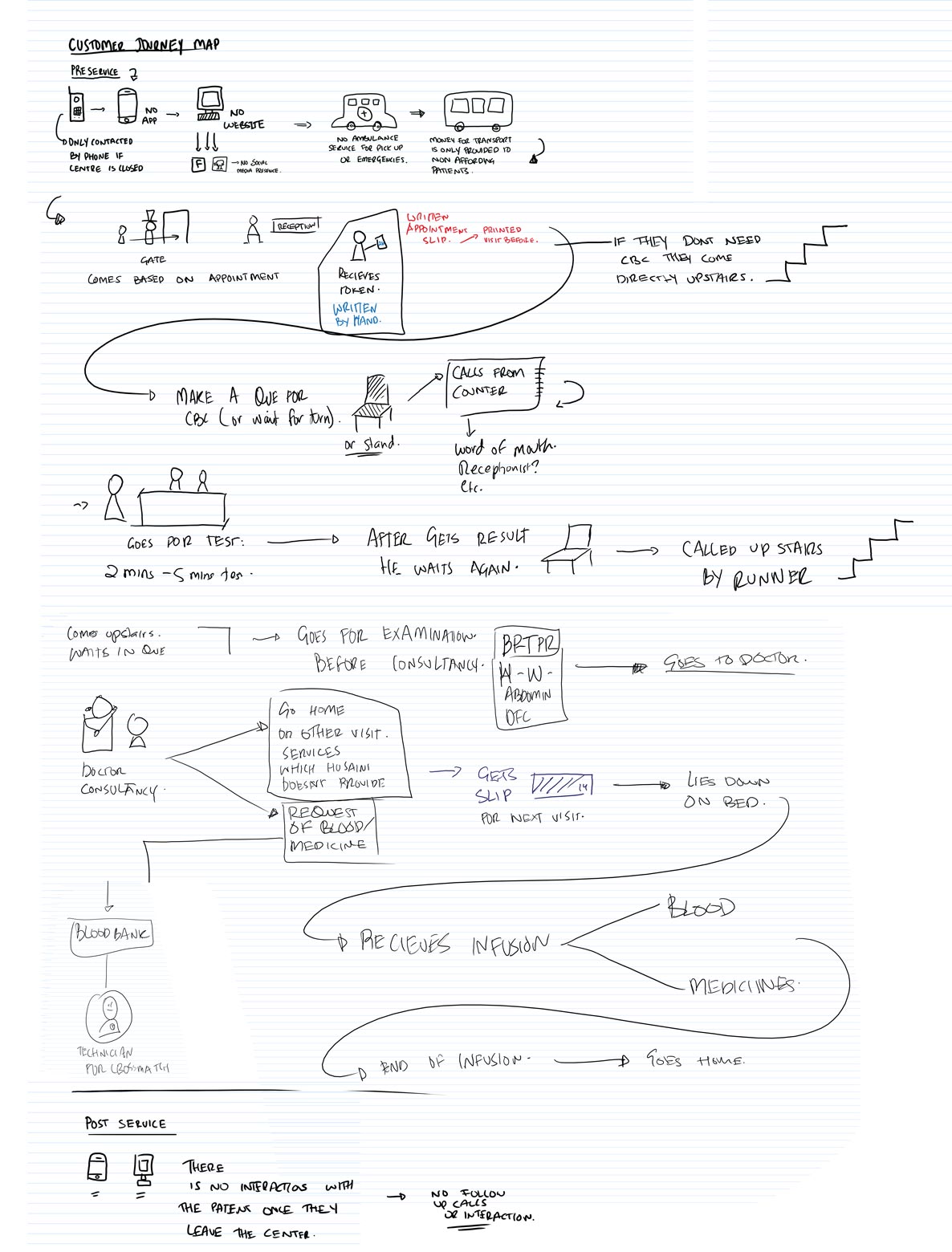
Figure above shows the journey of patient through the center.
Key Learnings:
- ● There is no interaction with technology (mobile, web).
- ● Patients are only contacted in time of emergencies.
- ● There is no pick and drop service.
- ● There is a lot of wait time between each touchpoint.
- ● Most patients are called by word of mouth to the CBC test and upstairs to the center.
- ● Some patients go upstairs without being called.
- ● The blood bank has its own procedures for preparation of blood which need to be examined and mapped.
- ● There is no interaction with the users once they leave the service.
Limitations: One may understand the journey the user goes through during the service at each touch point and assume their emotions and behaviors, but not until one truly speaks or views them in the real context of the service can we truly understand what they are actually feeling. In our experience we did not map the emotions felt at each touch point, this is something we could have done differently.
Service blueprints
The service blue print is created to see each detail of the service. It helps identify what happens in the back end as well as in the front and the points of intersection. The blue print shows each persons responsibility in the provision of the service (Stickdorn and Schneider, 2011).
In order for us to map this blue print we had to understand how the blood bank, laboratory and thalassemia center were working in relation to each other. It was essential to speak with every staff member for this process to come together. It helped us identify where our speed bumps were and how we could make our service smoother.
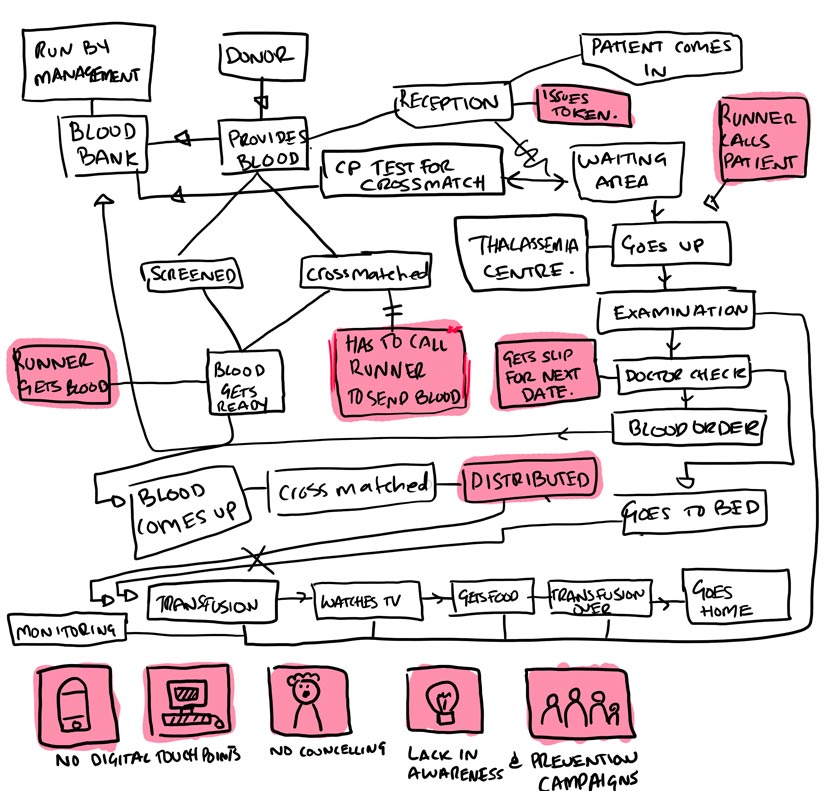
The above figure is the service blue print of the center. It shows the relationship between the bloodbank and the thalassemia centre. We can see what processes are taking place in the back end. The boxes highlighted in pink represent opportunities for improvement within the service.
Journey of Blood

This figure represents the details of how the blood is prepared before transfusion.
Journey of blood from donor to patient
This video represents the journey of blood. First the donor comes and donates blood. The blood is then taken to the lab for testing and cross matching for the patient. Once the cross match is done. The blood product is prepared. The runner is than called from the second floor to come and get the blood. Once the blood reaches the second floor it is distributed by the nurses. The verify the details of the patient and blood and then it is transfused to the patient. The patient then goes home.
This video helped us understand and gain insights that were not seen before. It showed movement and flow of several users and the product it self. I would introduce and use this tool in future projects as well.
Key Learnings:
- ● It is difficult to communicate with the runners.
- ● The runners in the blood bank needed to be found physically.
- ● The blood goes between rooms by the technicians and not the runners.
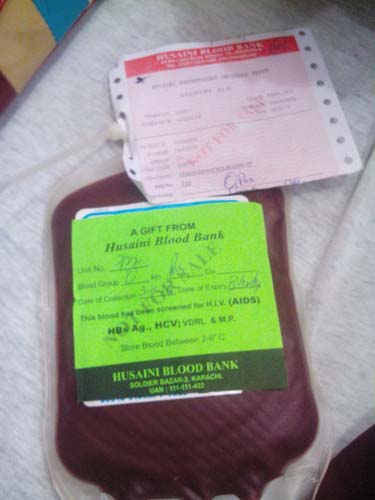
- ● Slips are separate from the bags.
- ● The runner from the 2nd floor needs to come down to the blood bank more than 5 times a day.
- ● Runner has to physically call patients up stairs.
- ● Slips and tokens are all paper based.
- ● General lack of digital technology.
- ● Patients do not receive counselling.
- ● There is a lack in Thalassemia awareness and prevention campaigns.
- ● The donors never meet the patients.
Limitations: It is very important for the senior managers to be involved in this process as not all staff members know each and every interaction between the stakeholders. Certain interactions can also not be disclosed about what happens behind the scenes. This may lead to an incomplete blue print and lack of data. An animated video journey may not be able to be produced by everyone.
Storyboards
Storyboards are a visual representation of how a sequence of particular events of a service come together. It can also be used to visualize hypothetical situation of a new service. (Stickdorn and Schneider, 2011) It helps us better understand stories and customer journeys.
We did an entire walk through of our service, but not until we visually represented it that we learnt many aspects of the service.
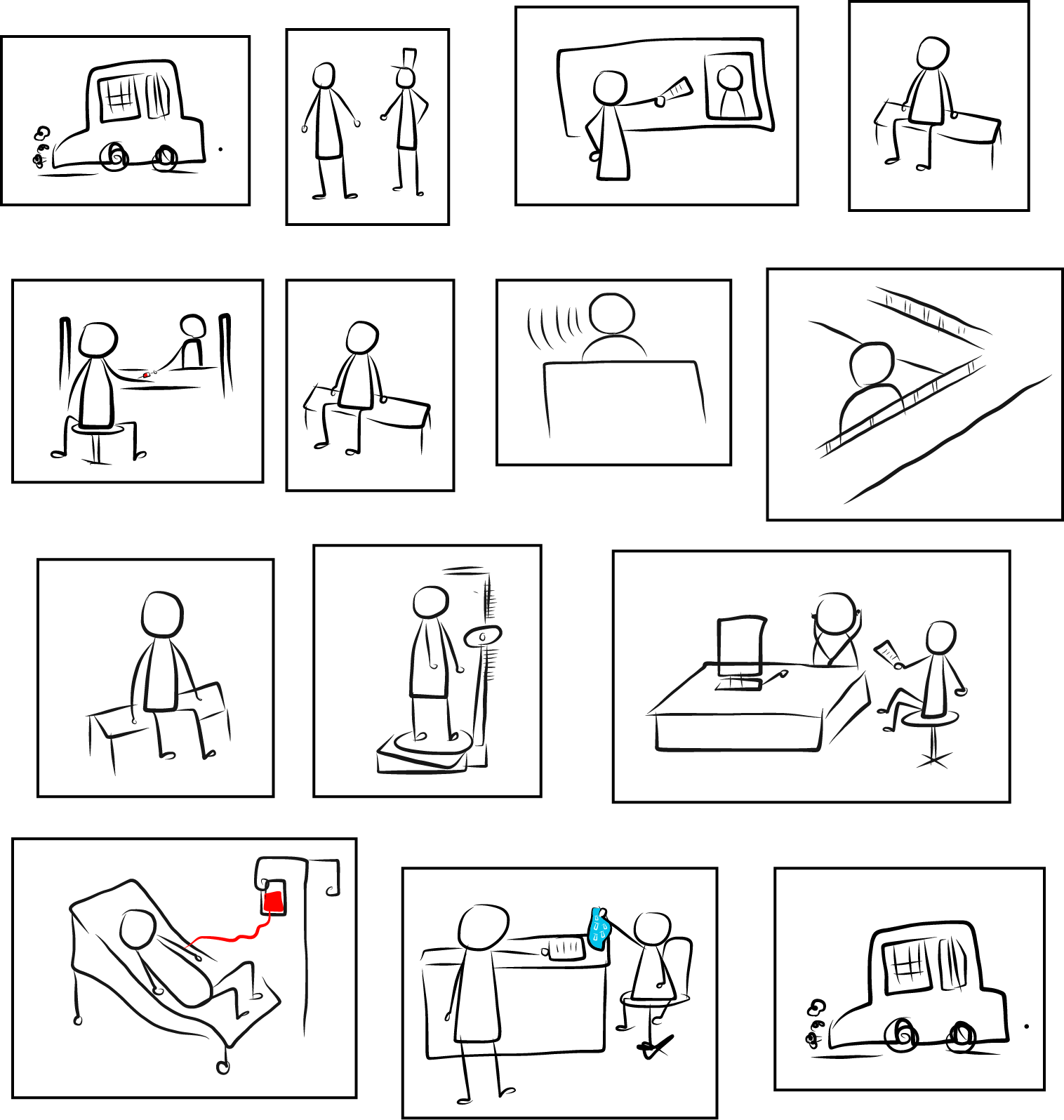
Key Learnings:
- ● The patient had to use a paper slip at each touchpoint, and it could easily get misplaced
- ● The patient had to wait between several touchpoints of the service.
- ● The runner had to shout for the patients to come to the second floor.
- ● Plastic bags were being used to give medicines to the patients.
- ● It made us question what was the feeling of the patient at each touch point, and what did they do during the wait time?
Limitations: Not everyone can draw. It may be time consuming.
Contextual Interviews / Shadowing
This section we will cover two methods, Contextual Interviews and Shadowing. The reason I decided to present them together in this section is because both methods compliment each other and the findings were quite similar.
Data was also gathered using printed sheets, journals and digitally using a Wacom Cintiq Hybrid Tablet, photographs and videos.
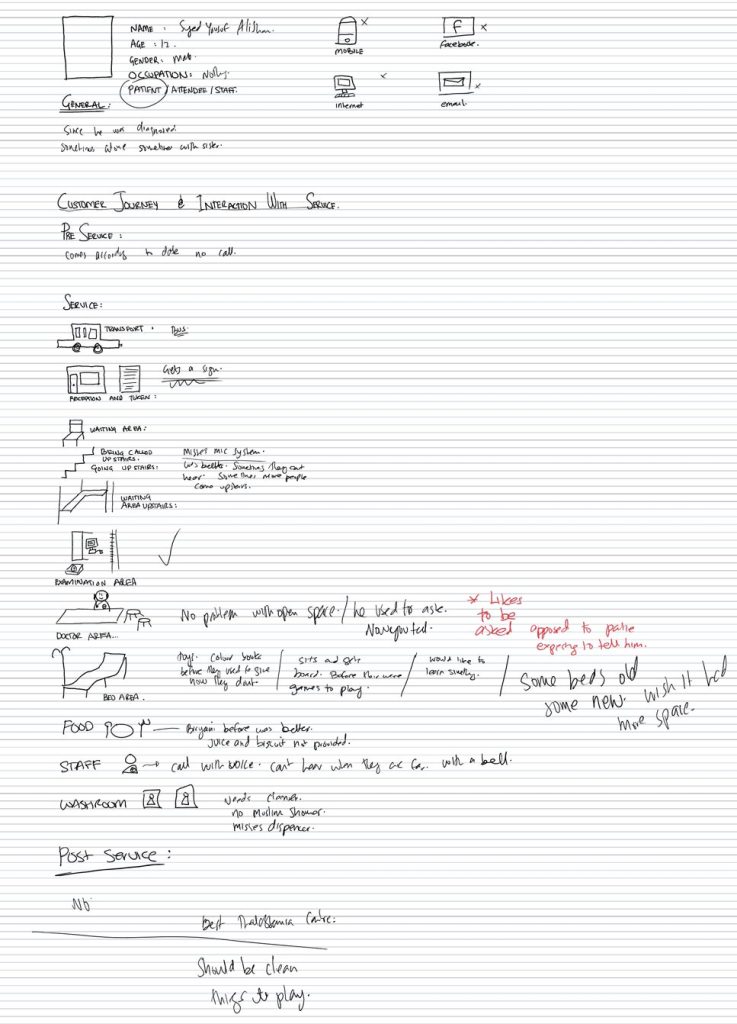
Example of how the data was captured during the interviews.
I will now show and explain the problems, insights and opportunities the Thalassemia Center faces from Preservice, Service to Post service. In some sections these will be listed, as they are straight forward whilst in others they will be explained in detail. Several of these insights have been addressed and you can see them in the Solutions section.
Preservice
Currently the only contact the patients have with the the service before they get to the center is through an appointment slip which they are provided during their last visit and if the center is closed for any reason.
There is no contact with the web or mobile.
Service
Transportation and Way Finding
- ● There are strikes in the city due to the rise in price of CNG and Oil.
- ● Political parties protest and have Dharnas(Occupy areas)
- ● During the first 10 days of Mohurrum.(Religious month of Islam)
There is also no pick and drop service for the patients. When staff is picked and dropped, the driver usually does not go to their houses but gets them from a certain area. At times it is difficult for staff members to reach those areas. There is no stand by ambulance and the center in case of emergencies.

Road block to at the enterance of the main road to the Thalassemia Center during the first 10 days of Mohurrum.
Entrance and Reception
- ● There is no one to welcome you at the entrance.
- ● The security guard barely checks who is coming in and out.
- ● The metal detector does not beep.
- ● At the reception the patients are given a token number which the receptionist writes on their appointment slip.
Waiting Area
- ● A patient waits an average time of 10-15 mins before CBC test and 15-20 mins before going to the second floor.
- ● Limited amount of seating.
- ● Shared seating of blood bank and thalassemia center.
- ● No Tv
- ● No clear indication of who is a patient.
- ● No separate seating area for patients.
- ● No separate seating area for women.
Women complained about men who were not attendees of other patients. They said that other men would give them dirty looks and give cheeky comments. This would make them uncomfortable and they would go up to the center. We investigated this issue and we realized that many people who sat on the seats were accompanies of people who came to donate blood

Being called to the Second Floor
- ● Problem hearing person who calls the patient up.
- ● No indication of how many patients have gone to the second floor.
- ● If one does not hear they call they automatically go upstairs, this causes congestion on the second floor and it is difficult to control the flow of patients.
- ● The office assistant/runner has to scream from the second floor.
- ● There is no one stopping the patients from going up stairs.
- ● There is no one in charge downstairs
The office assistant/runner himself is a patient. He often has to go up and down the stairs to call the patients. This makes him tired.
Examination Area
- ● Need for better measuring tools.
- ● Readings are incorrect sometimes and it frustrates the doctor.
- ● Examination area is right next to the doctors area and the doctor gets disturbed.
- ● There is no calling system, or indication of whos turn it is.
- ● Some patients skip the examination.
- ● Examination area is not private.

Examinations are happening in the public.

The nurse is having difficulty checking the height. She is also using a ruler to tally the height. This may give in accurate readings.
Doctor Area
- ● No private room for the doctor.
- ● There is no lady doctor and 60% of our patients are women.
- ● There is a lot of privacy problems. Patients can not talk openly about their issues.
- ● The area gets crowded
- ● Patients break the cue and go straight to the doctor with their reports.
- ● If patients come without an appointment they need to get a slip signed in order for a token to be issued to them
- ● Some patients go directly to the doctors area before examination.
- ● Some patients said they like the open space so they can see the doctor.
- ● Some patients over hear what other patients say. They then repeat what the previous patient said in order to get extra medicines.
- ● A patient said that they like the doctor to ask them questions as apposed to the patients telling the doctor what their problems are.

From this image you can see that there is no room for the doctor. The examination are is right next to the doctors room. There are two doctors sitting on the same desk. Their are multiple patients near the doctors area.
Bed Area
- ● There should be space between the beds.
- ● Patients complained about smelling other peoples feet
- ● There should be a flat screen with organized programming for the patients
- ● Mostly people watch tv or play on their mobile
- ● Tv is Small can’t see the score
- ● Bed should be longer.
- ● Have to shout for attendies
- ● Would like some games
- ● Some TVs do not work
- ● Would like if the patient could learn something
- ● Some people come and lie down without their tokens – Staff Member
- ● Before patients were asked if they wanted entertainment. Now patients have to ask for entertainment
- ● Some like to talk with their friends
- ● Should be a curtain for the ICU unit
- ● Has a problem when pricking the patients because he has to bend down.- Nurse
- ● Expected that beds should be clean.
- ● Pillow and blanket would be nice.
- ● Separate beds for women
- ● Aircondition problems in the summer time
- ● Have to wait a long time for the blood to come
- ● Beds should have numbers
- ● Sometimes patients share beds.

Multiple female patients on one bed. Not enough stands.
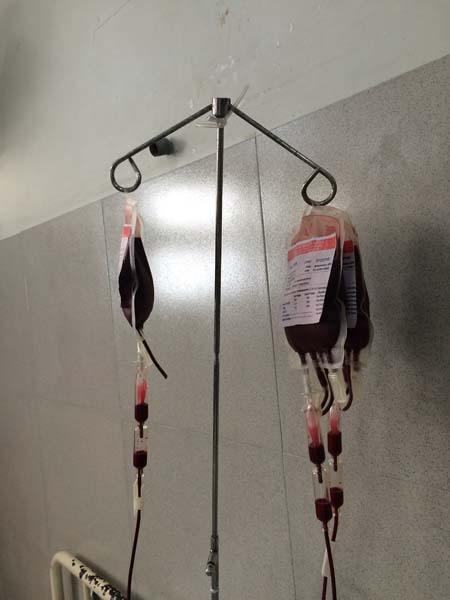
Multiple blood bags hanging from the same stand.

Very old and heavy Tv. Feels like it will fall out of the wall.

Patient can not fit on the bed.

The ICU unit is behind the two doctors. There is no curtain. There was an unfortunate death at the center a couple of weeks ago and many patients had to witness it with their own eyes. It was very disheartening.

The nurse is required to carry her medical supplies in her hand from station to station.
Patient hitting the TV to try to make it to work. Possible hazard of it falling from the ceiling and someone getting hurt.
Food
- ● The food is not good.
- ● No consistency in the quality.
- ● Cutlery is not provided, patients have to ask for it.
- ● No Variety in food.
- ● No liquids provided with food.
- ● Some bring food from home.
- ● There used to be chicken in the biryani before now there isn’t any.
- ● Patients often order food from the runner or Saqib another patient.
- ● Juices used to be provided before.

Patients eating biryani with his hands.
Washroom
- ● Washrooms are not clean.
- ● No water in the washrooms most of the time.
- ● No soap dispenser.
- ● Need a proper hanger for the blood.
- ● Smell in the washroom.
- ● No muslim showers.
- ● Very Dirty.
- ● No hand dryer.
- ● Liquid Soap Dysfunctional.
- ● Public washrooms do not have a commode.
- ● There should be a separate washroom for females.
- ● No dustbin in toilet.
- ● Patients carry blood bags by hand to the washroom.

Washroom is dirty. There is no muslim shower. The flush is often broken as well.

This is the staff washroom. It was very dirty
There was no water running in the tap.

No handicap support for patients. Some patients are so weak they need to be carried.

Soap dispenser was not working. Bars of soap were kept in the plastic cup.

Stair case is rusted.
General Cleanliness
The center was quite dirty from the outside as well. Here are a few images to illustrate the situation

Pan spit at the entrance of the center.

Junk on the first roof.

Pan spit on the walls near stair case.

Stagnant water on roof mixed with pan spit.

Junk on the back side of the roof. It is not visible unless you walk around the corner. This can be a fire hazard

More pan spit and trash.
General Space

The nurse is sorting all the blood bags on the office assistants counter. The office assistant does not have enough space to prepare for Desfrol medicines for the patients.

Attendee preparing Desfrol injection for the patient on the office assistants desk. There is no designated area to prepare this medicine.

3 doctors are sitting on the same desk while one of them is attending to the patient.

Many attendees in the bed area.

Office assistant preparing medicines.

Office assistant/Runner eating food in the examination area behind the doctors desk. No designated sitting area for staff.

Desk set up in the middle of the waiting area that has nothing to do with the Thalassemia center. This desk took up many spots that patients or attendees would usually sit on chairs at.

Attendees standing as there are no places to sit.

Rush in the middle of the center.
This video shows attendees and patients moving in and out of the bed area. I asked the office assistant what she thought, and she just smiled at me. The floor manager said that it is difficult to maintain the flow as many of the attendees like to give their children food and sit with them. They also dislike sitting downstairs in the waiting area.
Identification of Service and Staff
There is no signage any where in the whole building indicating where the center is. There are no signs anywhere in the entire premises. Most staff members do no have uniforms. It is very difficult to identify who is a patient who is a staff member.

No sign to indicate entrance of center

There was no Push or Pull sign at the entrance. Every morning I would come and attempt to pull the door and would not ever get in on the first try. The office assistant heard me complaining and noticed my frustration. The next morning she put up a Post it. These little things make the service better.

Make shift push sign on the entrance door.
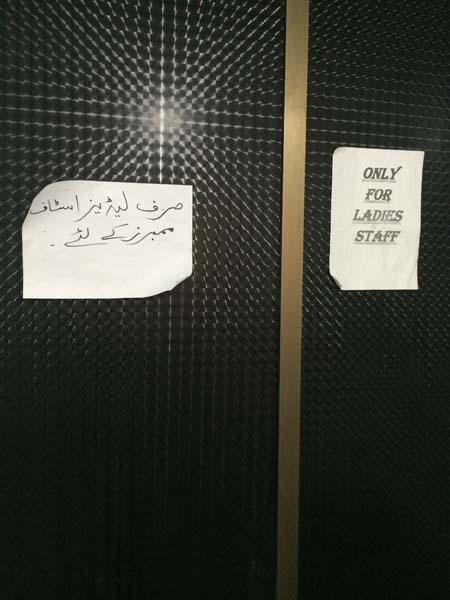
No proper signage in toilets.
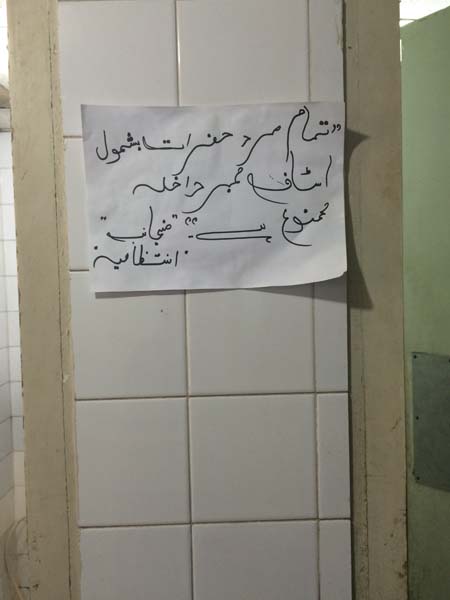
No proper signage in the toilets.

Staff members do not have uniforms. They are hard to identify.

Doctor did not have uniforms as well.
Additional Insights
In this video you can see that the office assistant is looking for the runner. It has already been 10 minutes since the Lab technician has informed the center that the blood is ready for pick up. The runner walks in from the back door and the office assistant does not see him. She tells asks the janitor where the runner was. The janitor spots the runner come in and then tells him to get the blood.
In this video you can see the journey of the runner as he gets the blood. As he is a patient he is tired from his last task, which was to get tea for the doctor. Many of the staff members do multiple jobs. This staff member is in charge of maintaining the flow of the center, calling the patients, and getting the blood from downstairs. Once reached downstairs he makes a sarcastic remark and says “look there are so many bags here”. There were only a couple of bags, and he complained that they always call me down and there aren’t even that many bags. He then dumps all the blood bags in the box and the slips gets jumbled up, which the Lab technician had organized earlier. In the prototypes and solutions section you will see how we improved this process.
This video showing how the nurse cross matches the slips with the blood bags before distributing them. She did not know that the lab technician had done the same job 5 mins prior to this.
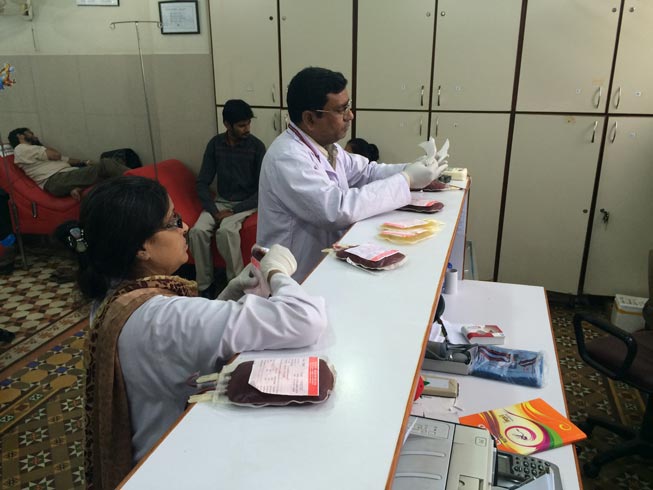
Sometimes two nurses are needed for the same task of sorting blood slips.
This video on the right shows how the nurse distributes the blood bags. He has to identify each patient by their names. He calls out to them as he moves around the room. Many patients are sleeping or are in the other room. He has difficulty finding them and handling the blood bags. The patients also get disturbed when he calls out other patients names loudly.
Interview with the Lab Technician:
I visited the Laboratory to understand how the blood was being prepared and spoke with the Lab Technician. It helped in identifying many of the behind the scenes activities that were not seen on the customer journey but could be incorporated in the Service Blue Print. What I learnt from her was that she had to always find the runner on her floor to move the blood from one room to the other. There is no way for her to track him so she would often just transfer the bags her self to the product maker. Another insight I got from her was that she would cross match the slips with the bag and then send the blood bags and slips separately to the second floor. Once the blood bags reached the second floor the nurse would repeat the same procedure as the lab technician. So basically the same job was getting done twice, and because there was no communication between the two staff members they did not have a clue.
Interview with a new Doctor:
One of the doctors at the Thalassemia Center had recently been hired. He had come at the same time as the start of the project. As he had not been working there before he had a fresh pair of eyes and noticed things that many other staff members and patients had not seen. Here are the insights I got from him:
- ● He did not know that Husaini Blood Bank had a Thalassemia Center until he got the job and came to the location.
- ● He went on the internet to find out more but there was nothing there.
- ● He liked that patients were also staff members.
- ● He had trouble using the software and no proper training was given to him.
- ● He believes that there is a general lack of staff.
- ● He thinks that there should be better equipment to monitor the patients.
- ● He commented on the cleanliness of the center, the noise, and security.
- ● He said new patients and staff members need to be trained about safety procedures.
- ● There was no place for him to sit and eat.
- ● No hand sanitizers.
Interview with an Intern.
I spoke with an intern who had come to work at the Thalassemia Center for 15 days which was part of her training. She also had a fresh pair of eyes which was great. I was hoping to find out more about the patients but to my knowledge she shared something completely different. I was fortunate enough to speak with her on her last day of work so she felt open to share her experience with me. She stated that she did not get much experience or training working at the center. She only pricked 3 patients in the time that she was there. That is significantly low considering there are 30-50 patients who come in daily for transfusion. She felt as if the nursing staff was treating her like a helper as apposed to a medical student. They mainly asked her to cute tape for them. There was no senior in charge of her for guidance. She did not raise these issues with anyone in fear of conflict. She said she learn a lot from working on the first floor at the Blood Bank but not much at the Thalassemia Center. She said that there were at least 20 other interns who came to the center prior to her and felt the same way which was quite shocking.
Group Interview with women patients.
A staff member and myself had the pleasure of being able to talk to a few patients who were women in a group. This aided in their comfort level as they could build on each others discussions and were more open to expressing themselves. They were very lively and often made jokes about the center’s problems, but when asked on a serious note they shared openly and in detail. Many of their insights had been covered above. I would like to highlight some additional key insights:
- ● The girls would usually come in groups and try to get appointments on the same day.
- ● Some of them would come also if they did not have an appointment to give company to their friends.
- ● They insisted on wanting a lady doctor and a separate room for the doctor.
- ● They loved a previous lady doctor who was no longer with the center.
- ● They were willing to pay for food, as apposed to getting the one they received at the center.
- ● Commented on limited stands.
- ● They missed old staff members and wish that they would not change.
- ● There is a lack of awareness programs.
- ● There were no more picnics and seminars.
- ● Sometimes the center is like a fish market.
- ● They would like to get medicines on location.
- ● Wish there were activities that the patients could have.
- ● There should be a full service Thalassemia hospital.
Group Interview with Staff Members.
Group interviews with staff members began at the very start of the project. We sat together for a couple of days together after work hours for a couple of weeks. We analyzed every touchpoint they were having with the service as well as the patients. Many insights are listed above, but I would like to mention some additional ones. They are:
- ● There is no regeneration for lost tokens.
- ● The patients has to wait till 9am for the doctor to sign of on a slip to get token if they come without an appointment.
- ● Patients sometimes trouble the doctor by calling at odd hours.
- ● Due to the increased number of beds the doctor’s room was removed.
- ● Access to medical history of patient is only available for 1 year.
- ● Patients who are not part of the center delay the flow.
- ● Some patients who are not Thalassemia and come for check ups.
- ● Sometimes blood bags come without the slips.
- ● Some patients speed up the flow of the blood them selves. They need to be made aware of the risks of that.
- ● Difficulty in finding the veins sometimes during pricking.
- ● No emergency bell in the washroom.
- ● No proper disposal of needles. Janitors have been pricked during clean up. Serious safety problem.
- ● No system for missed appointments.
- ● No automatic messaging system.
- ● No replacement staff on call.
- ● Maintenance department does not respond when things need to be fixed.
Group Interview at Thalassemia Federation of Pakistan Conference.
I personally went to a Thalassemia Conference held in Lahore to speak to patients and service providers of other Thalassemia Centers across the nation. I did this as I wanted to learn what other centers were doing for their patients and how it compared to ours. You could say it was some what like a service safari but not exactly as I was not examining or experiencing another service. Some finding were very shocking whilst others gave great insight to how we can adopt it to our service. Here are my findings:
- ● Some centers used blood bags made in china which caused serious health issues and in extreme cases caused death.
- ● Some centers have a system where the patient has to come a day earlier to do his CBC test for cross match and then receive blood the next day.
- ● Agha Khan Hospital has car parking and valet system. They have digital counters for blood tests. They have three options for rooms, a ward, semi-private room or a private room for transfusion. They have a bell system to call nurses but sometimes they take a long time to come. There is no response feedback system to know if they nurse has heard you or not. Might be troublesome in times of emergency. Agha Khan is not free and treatment there is very expensive.
- ● In on center you have to wait 30mins-1hr before going in for a CBC test. At Husaini Thalassemia center you wait only 5 mins-10 mins.
- ● Some centers do not make patients and families that aware of the disease.
- ● Some centers give limited on no Desfrol to the patients for iron chelation.
- ● Some centers require a replacement donor for patients.
- ● Some centers do not have sufficient beds. Patients have to sit on chairs or stand sometimes during transfusion.
- ● Some centers do not have a cueing system.
- ● Most centeres do no have proper cross matching and screening systems. Patients often get HIV and Hepatitis C after transfusion.
- ● Most centers do not provide any food or snacks to the patients.
- ● General lack of government involvement in Thalassemia Care and Prevention.
- ● Patients said that there should be awareness campaings like they have for Dengue and Polio.
- ● In some centers you need to call before hand to find out for availabilty of blood.
After going to this conference I realised that our center was very good. If we did not provide much additional facilites we atleast provided safe and clean blood and proper iron chelation treatment which is essential for the survival of the patients. I also learnt that Desfrol is not given free of charge to all our patients. Some patients have to purchase it them selves. It is only provided to those patients who can not afford it at all. Also the dose provided is not of the optimum level. The organization claims that it is giving more than any other service and that other services are only trying to keep the patients alive.
Feedback and Reflections on this Process.
Many stakeholders took place in this process of being interviewed and interviewing others. In the group I asked them how they felt and what the expected before these tools were introduced, how they felt now and what they hope for the future. Some were asked to just give general feedback. Here are some responses:
“Why are they calling me and involving me in this meeting? I feel happy now as I see that problems are getting solved. I hope that the management was like you and had more discussions to discuss our problems. I really hope all our problems will get solved” – Office Assistant/Runner.
“I thought you were some english man, and wondered why I was in a meeting? I feel that something good is going to happen now.- Female Office Assistant.
“During the first meeting I was a little uncomfortable. I did not understand english. I felt respected and involved when you invited me to the meeting. I hope everything is good but I do not know about the future” –Female Janitor
“I felt good being part of the meetings, It feels like you are going to do something. If things get implemented it will be very good” – Male Janitor
“What we are doing is good for the patients and organization. Patients come first. Omid(hope) has come in front and improvement is coming. I liked how we are involving the atmosphere. I enjoyed talking freely. I want these discussions to continue.” Doctor.
“The interviews helped to assess our service, understand the current experience and level of satisfaction of our patients. The paper guide helped cover all aspects of the service” -CEO
” The questionnaire was comprehensive and covered all basics of the service, problems and pressure points. Patients have problems and their messages do not get through. Questions were on a micro level. The patients should also be interviewed by external people. Due to the massive expansion of the Blood Bank it has caused negligence towards the Thalassemia Center.”-IT Manager.
I personally learnt that talking to the patients and the staff was a great experience in gaining insights. They felt more comfortable talking to me as I was someone external. Some staff members and patients said that they were scared that they might not be part of the service if they complained. I told them not to worry and that their information was confidential and would be anonymous. They could also withdraw from the exercise if they liked. They also said that what would happen after I left. They enjoyed having group discussions. They said in the entire history of the Thalassemia Center, not ever has everyone sat together to ever discuss anything. They wished that the managing trustees could also be present in future discussions or visit the center and ask how things are operating.

First group session with the staff members.

Intern interviewing a patient. It was very helpful that the intern was a female as the women were more comfortable sharing their stories with her.

The CEO interviewing an Attendee.
Limitations: Different people may see different things. One may be looking for something particular and may over look something else. Users may not always tell the truth. It is up to the interviewer how much in depth they want the interview to go. Questionnaires may not cover every aspect of a service. Both tools are time consuming, and need to be done over a significant number of hours. Budgets and time frames may not allow full use of the tools.
Mobile ethnography
Mobile ethnography is defined as an ethnographic research. It takes place independent of the researcher. By providing the user with a camera allows them to gather user centered information. They can choose themselves which touch points they would like to highlight.
At the Thalassemia Center we asked one of our patients to capture her journey of the service. As she had a smart phone it allowed her take photographs where ever she wanted. After she took the photographs we transferred the files to the computer and asked her to talk about why she took each picture and what it meant to her. This gave us certain insights that we had not seen earlier. It really felt as if we were experiencing the service through her eyes.
I will show her journey and comment on our learnings with each photograph.

Patient arrives at center and goes to the reception to get her token.

Patient receives print out of test result.

Patient describes the rush in the waiting area. There are limited amount of seats as well.

Patient prepares Desfrol injection on the bed.
From this image we learnt that there should be a specific area for preparation of Desfrol.

Table was placed in the middle of the waiting area. This caused flow problems for the patients and the staff.
Blood bag and slips are crossed matched.

The nurse carries her tray with her to each station
Patients enjoyed making drawings.

The nurse cross matches slip and comes to check on the patients from time to time.
Patient receives new token and is thrilled with the heart shaped prototype.

Patients and attendees in the waiting area.
From this we learnt that some patients enjoy doing crafts as they wait.

Cleanliness problems in the waiting area. There is empty spaces there as water drips from the top water tank.

Patient getting examined. No private examination area.

Patients shows the center with the new token system.

Multiple items hanging from the

Patient being pricked. Patient also talks about how some staff members are more experienced than others.

Patients requested the runner to bring breakfast for them.
From this we learnt that there is no proper sitting area for patients.
Patients like getting food, and wish there was a canteen.

Patient showing how the food came. She also describes how the quality of food is not as good as it used to be. Also cutlery is not provided.
We learnt that there should be more variety of food and better presentation when provided.

Patient getting a CBC test done.

Patient sits on the security guard’s chair.
From this we learnt that the security guard was not present at his postings
Patients also took seat due to limited amount of chairs in the waiting area.

Patients result of the CBC test.

Patient shows multiple doctors on one table. The patient also told us that there should be a room for the doctor as they cannot discuss their private concerns in public. They also wished that there was a lady doctor.
We learnt that we need to address this issue as 60% of our patients were female.

Floor managers and office assistants desk.

Nurse preparing to prick patient.

Multiple items hanging next to the blood.

No proper sitting area for refreshments. Soon after this picture was taken the tea spilled all over the bed.

Patient shows that her blood is almost transfused
Limitations: The researchers or users may not have access to cameras or smart phones. The user may take pictures of someone without their consent and it can be un ethical, unless they get consent. The user only takes pictures of what they want to show, other aspects of the service may not be captured.
Storytelling
Storytelling is a method for sharing insights and new services.-Marc Stickdorn (Stickdorn and Schneider, 2011)
In our case we used this method when we were trying to gain insights from the patients and staff members. We had already conducted interviews so in order to make this exercise more engaging and fun we got the users to make drawings and tell their stories accordingly.
Below are a few of the images created with captions explaining what they represent or what the users said.

The patient describes his journey at the Thalassemia Centre. He talked about how he got hurt and came to the centre. You can notice from the character. He gets happier as his journey continues as he gets his transfussion and gets to watch cartoons on TV.
We learnt that sometimes little things like cartoons can make children happy and keep them entertained for the time they are at the center.
This story shows how Saqib delivers medicines to patients at home.
We learnt that the patients really connect well with Saqib. Even though he is not part of the center’s staff he still plays a great role in making the patients happy as he delivers medicines, food or whatever they need at home and at the center.
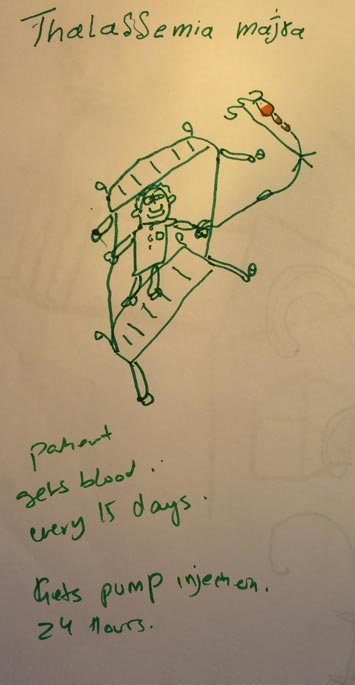
The patient describes how often he needs to receive blood. And that he needs to take the Desfrol injections everyday.
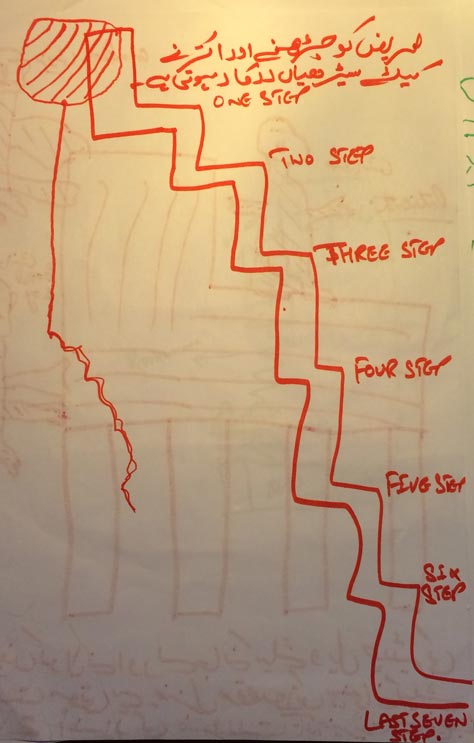
This was drawn by the janitor. He tells us about how he has to go up and down sometimes to get the blood when it is ready. He also says it would be nice if there would be a lift for the blood to go up on its own.
We learnt from this that staff members often do multiple tasks that are not necessarily part of their job description.
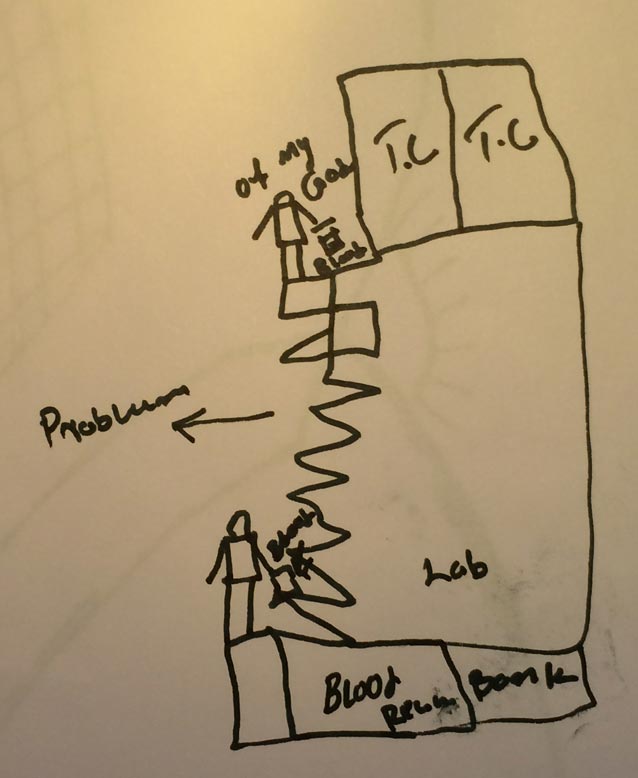
The office assistant/runner tells us about how he is a patient as well and gets very tired going up and down the stairs multiple times a day to get the blood for the patients.
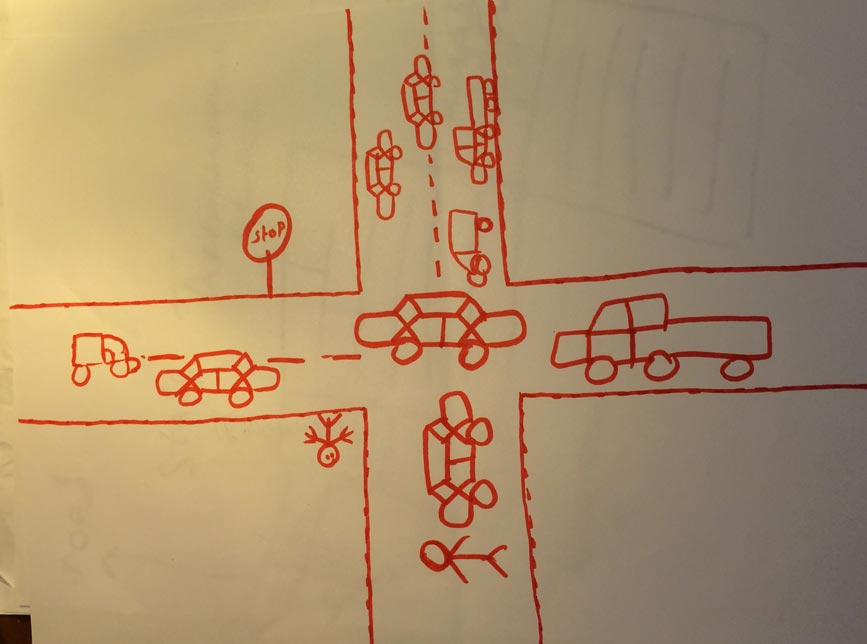
A patient describes how it is difficult to come to the center sometimes due to traffic jams, political rallies and religious ceremonies.
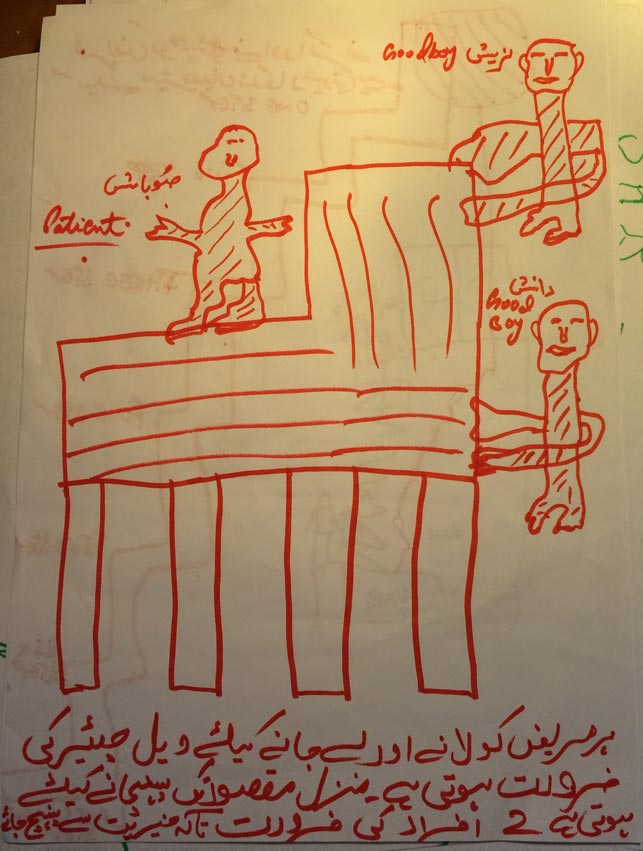
The janitor describes how we the center does not have a lift system and that some patients are in such pain that need to be carried up the stairs on a chair. He also writes how it takes two people to transport the patient downstairs and that it is very difficult sometimes. ( You may see a video of this in the shadowing section )

A patient describes how he is very content with the service and is very grateful.
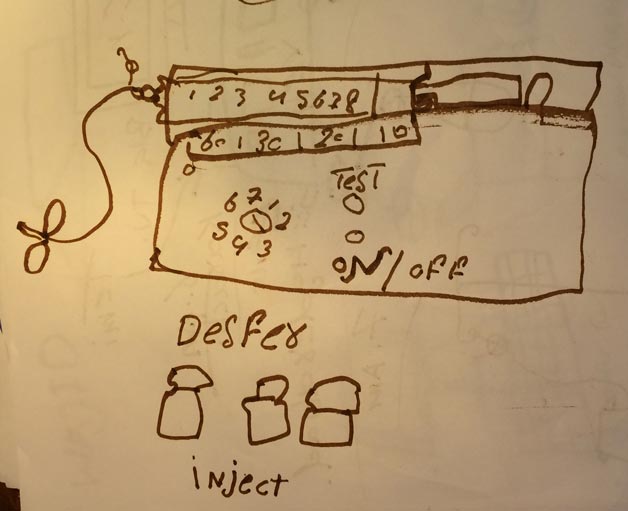
A patient talks about how he needs to take desfrol injections everyday to reduce the iron in his blood due to the regular transfusions he receives.
I personally learnt that taking this medicine is essential to the patients survival
A Day in the life
A day in the life helps us understand the typical activities a user performs in their daily lives. It helps us understand how they have interact with our service during the day and what they are thinking and doing outside the serivice. It gives us a holistic view of what drives and motivates them day to day (Stickdorn and Schneider, 2011).
I decided to interview Saqib Abdul Razzak about a day in his life from the last week.

Saqib wakes up between 9-9.15am. He showers every morning and gets ready for work. He eats his breakfast and leaves for work on his motorbike. He is a supplier of general items and medicines. According to his orders he takes his rounds of the market and locations he needs to supply the goods to. He goes to purchase the items, and usually gets it on credit as the store keepers trust him a lot. He buys his goods and then goes to the organizations. He supplies to organizations as well as the patients at the organizations. He begins at Saddar Kamal Hospital. He then goes to Husaini Thalassemia Center where he only takes orders from the patients, he spends some time with the patients and then continues his journey. He goes to Fatmid Foundation to provide general items, stationary and laboratory equipment. Then he goes to Haemophilia Society for general supplies and to take orders from the children. Goes to Dolmiya to purchase the items. After he supplies each organization he goes towards the airport to Quaidabad. Over there he repairs the Desfrol pumps that the patients gave him. Sometimes he delivers the medicines and pumps to patients houses as well. In the late evening he goes back to the market hoping he would get some orders over the phone. He enters his accounts into a journal he keeps with himself. He stays in the market till about 10-11pm. He then goes home and plays with his son in the park. He then gets ready for bed and goes to sleep.
Key learnings:
We learnt that patients love to have snacks at the center. Many of them wished that there was a canteen. After brainstorming with Saqib we proposed that we could have one of our cupboards utilized as a snack bar. We also believe that it is very important to involve and hire patients to be part of our center. It would be a great opportunity to involve Saqib in our purchasing department.
Limitations: A user may not be comfortable talking about another day from the life. A user may not come into contact with the service during his noted day.
Card Sorting
Card sorting is an exercise we adopted from IDEO’s Human Centered Design kit. It is a tool with helps engage in conversations about that is most important to the users. It also helps the researched identify what really counts as they ask the user to rank the cards in order of preference. It also helps to start deeper conversations about what they value and why. (Designkit.org, 2014)
We had conducted several interviews, observed patients and identified many insights and problems. We wanted to know where the largest problems were so we could figure out which problems to address first. As we gained more insights, we integrated it into our interview process as well. We decided to make some drawings on cards based on some aspects of the customer journey and other problems presented to us. Here are a few images of our process and results.

Example of how the cards were made.
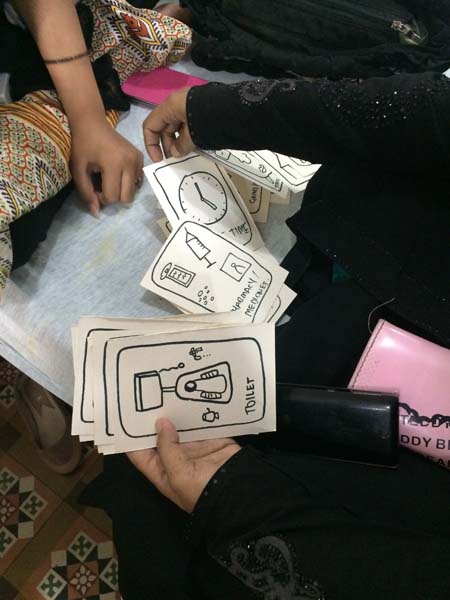
Patient sorting the cards.
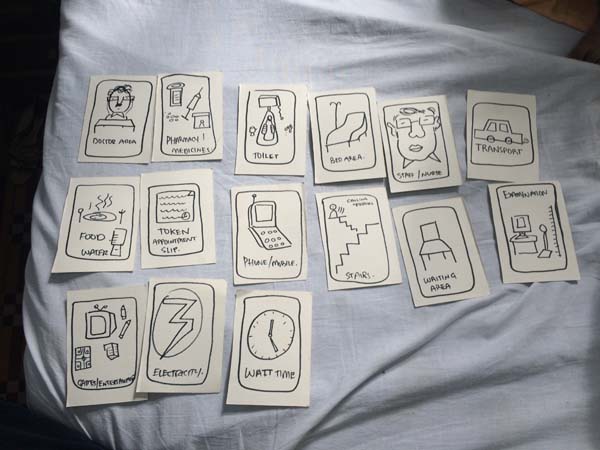

Sitting with patient using card sorting and contextual interviews at the same time.

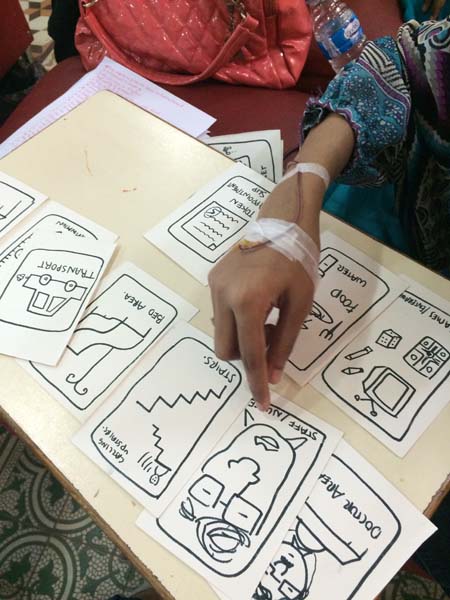


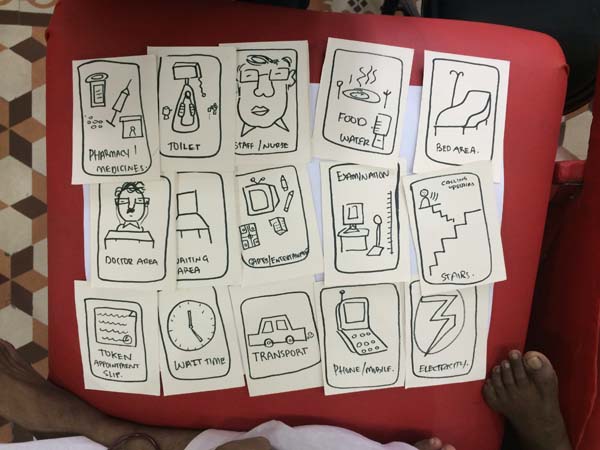
Key Insights:
After sorting out the data we figured that the major problems were in the following order:
- Doctor Area and Toilet
- Food
- Getting called upstairs and stairs.
- Nurses
- Transport
- Games and Entertainment
- Examination Area
We also realized that it took a long time to calculate the data as we had to physically count each scenario.
This patient walked by and was curious to know what we were doing. He thought it was a game and treated it like that. He was quick and quickly identified what he needed. He put games and entertainment in the number one spot.
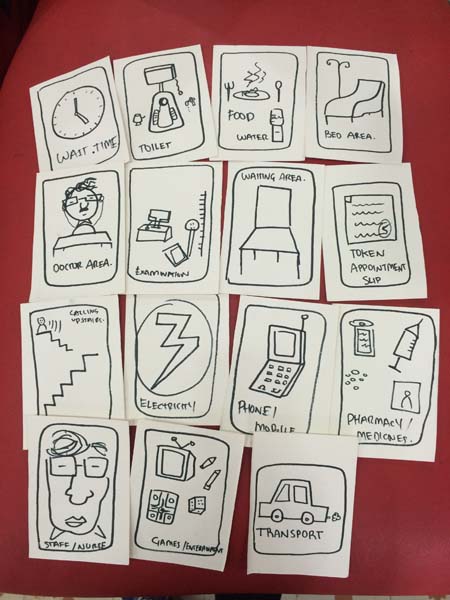
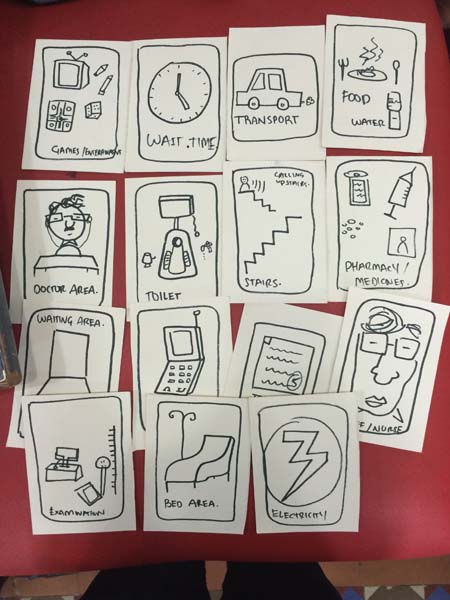
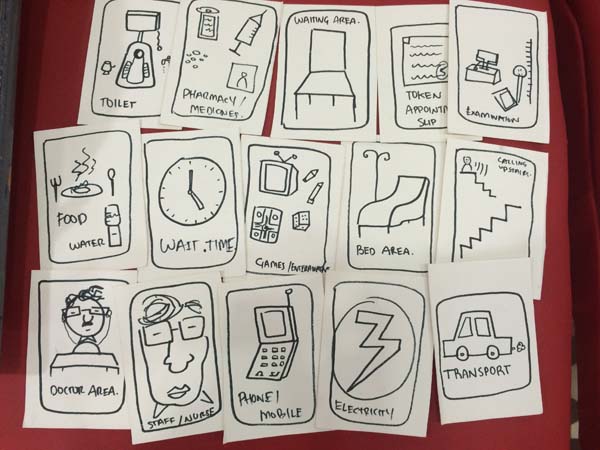

One of the staff members did the exercise and captured the findings on paper. We soon realized that capturing the results with a camera were great but how could we push it further. At the end of this section you can see how we iterated and created a new way of doing it.
Results captured in Urdu.


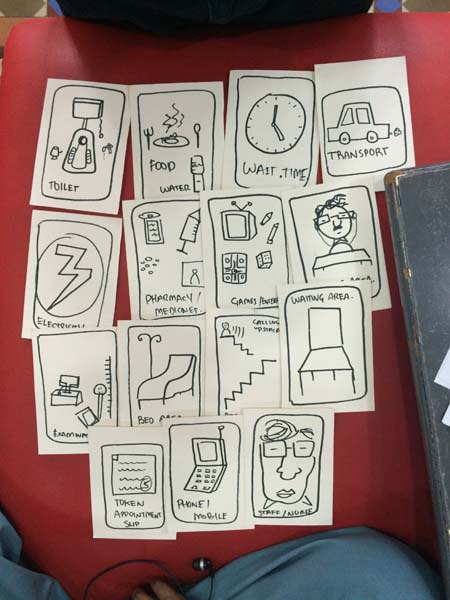
Feedback
“It was better than the interviews. It was quicker and patients were taking more interest due to the illustrations. It covered everything. There should have been a card about the infrastructure of the building itself. The patients talk to you when you talk in a friendly manner, not when you are formal.” – Intern
“It feels like a game. Putting it on a board will improve the process. I liked the fact that people are thinking about patients. I appreciate your work!” – Patient
“It is easier to understand and it prompts them to talk easily. If it was coloured it would be nice. As they are cards they can get dirty. Plastic coating it would be nice” -Office Assistant
“It easily highlights the aspect of the service. It makes life easier for them. It helps them recognize what to talk about. The cards should be in urdu” – Office Assistant/Runner.
Card Sorting Digital Prototype
I took in this feedback and for the next day I brainstormed about how I could make this process easier, to capture the information and keep the cards from getting dirty, lost and on a board. I looked for an app on the itunes store but could not find anything. I wondered to myself how I could make this digital. So I ended up scanning the images into the computer, and putting them on separate layers on photoshop. I then shared the screen of my laptop with an iPad and allowed the user to control the cards with their fingers. Here is the result in the video on the right.
It would very beneficial to actually develop an app like this. As it would help create which ever cards you want. It can help in adding additional cards. More than anything it would be excellent for capturing quantitative data so you may not have to go and physically count each result.
Expectation Maps
Expectation maps are created to figure out what the customers expect when they come in contact with the service. It helps the service provider understand which areas of the service need more attention than others.(Stickdorn and Schneider, 2011)
The way we carried this exercise out was to make the patients and staff draw what they expected from the service and the problems they were currently facing. Below are images of the their drawings with captions describing what they are or what the users said while drawing them.

Patient requesting ambulance service, pick and drop, prayer area, water in toilets, games and a better waiting area.
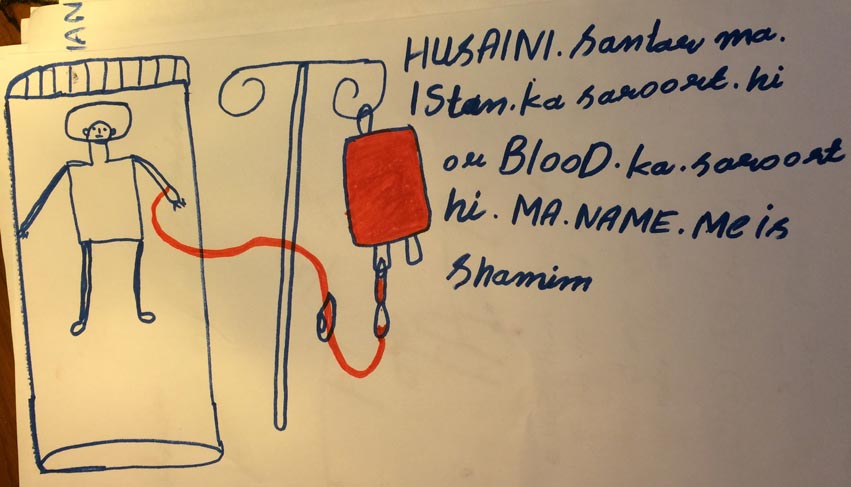
Patient requests extra stands for blood bags.

Patients would like to have a delivery system from our pharmacy. He likes how Saqib delivers medicines and other goods to them.
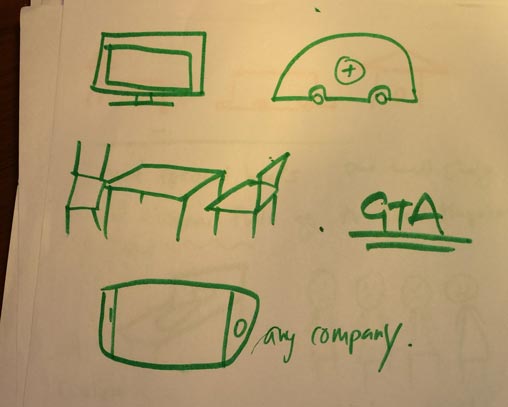
Patients wanted to play games, have better seating arrangements, a better TV and an ambulance service

A patients tells us how he enjoys drawing. He wishes that he could draw more. He said they would give them materials before but not anymore.
When I asked the staff about this they told me they still have the drawing equipment they just dont distribute it any more like they used to. They also told me that before there was a dedicated staff which would just interact with the patients.
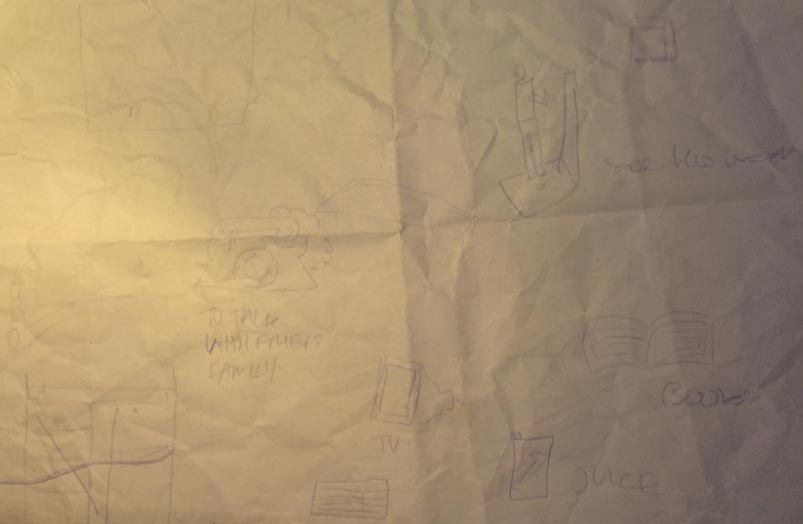
Patients requests a phone to talk with his family, books to read, better tv and juice. He also wishes that the examiner would tell him his weight.
This patient wishes for a canteen, sitting are, commode in toilet, better beds, better ICU unit and a sitting area.
This drawing was difficult to understand. What we took from it was that the patient wanted better entertainment on TV and toys to play with.

Patient requests better drinking water, a canteen for snacks, wifi and better entertainment.

This drawing was very powerful. It shows four patients being sent to another hospital due to that fact that the ICU unit was occupied.
It shows us that we need more emergency support and a standby ambulance for emergency reasons.
This patient wishes for drawing stuff and simply someone to come and speak to them. The patient also asked me what would happen after I leave. He enjoyed speaking with me and wish that other staff members would interact with the patients as well.
This patients wanted, better entertainment, a phone to call and a larger center.
One of the staff members presented an idea for a donation box.
We thought this was great as it would create a revenue stream for the center as well as create awareness about Thalassemia.

Patient drawing with is mother. Working collaboratively to draw out their expectations.
This drawing was quite insightful. We learnt that the patients currently shout to call out for help. This disturbs other patients as well as staff members. The patient suggested having a bell next to each bed. This would be helpful in calling the staff as well as emergency cases.
This patient wishes was a larger center.
The patient said he enjoyed drawing and wishes he could do it more. He also liked watching cartoons.

Another powerful drawing. This was made by the doctor. He tells us that we need a better ICU. The beds are limited in the space and that the there should be an oxygen machine and better monitoring devices for the patients. He says that the oxygen in the cylinders are limited.
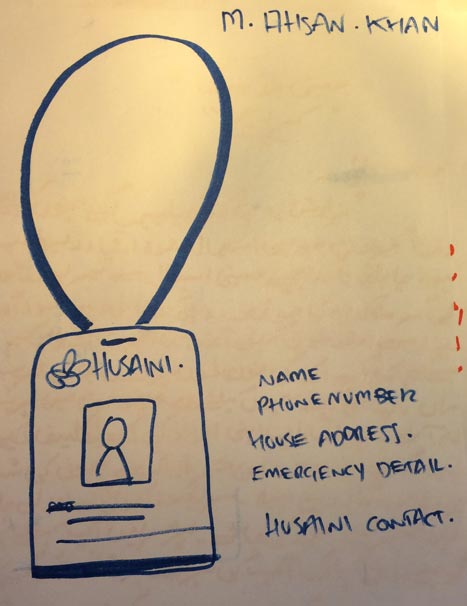
This drawing was quite insightful. The patient requests an ID card as he is stopped by police multiple times on the way to the center from interior Sindh.
Implementing this would help in identifying patients, for emergency reasons, and also for putting the patients blood group.
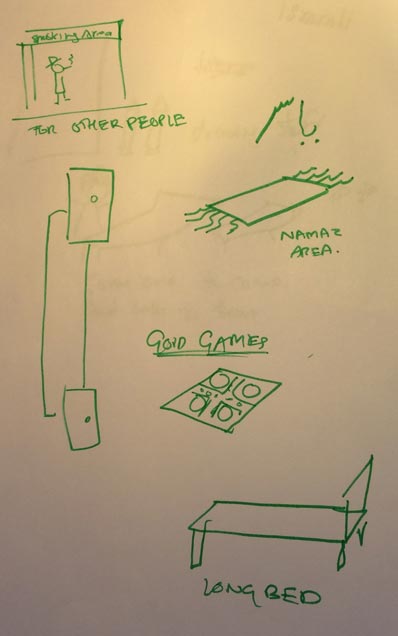
Patient requested games to play, prayer area, longer bed a lift. He also identified that there were people smoking in the waiting area downstairs.
The janitor decided to write a note instead of drawing. He writes that there should be a pick and drop service and that the waiting area should be improved for the attendees.
A patient writes her concerns. She said that the washrooms are not cleaned, there should be a canteen for snacks, they should not change the staff often as they prefer the old staff, often there is not drinking water, the food quality is poor, there should be a separate doctors area, there should be a lady doctor and that there should be a better air condition system like they have on the first floor.
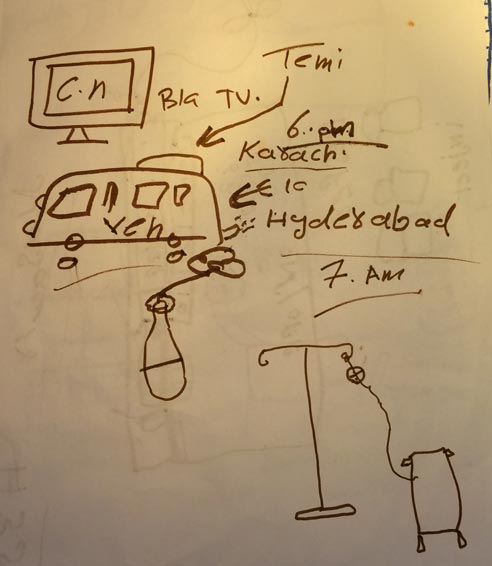
Patient requesting for a pick and drop. He talks about how much time it takes to come from interior Sindh.

Patient requests water in the taps, ambulance service, better waiting area, and better fans.

List of concerns 1
List of concerns 2
Patient happy drawing.
Patient drawing.
Limitations: Not everyone can get their message through drawings.
Service roleplay
Service role play is like a theatrical rehearsal method that helps generate ideas or helped during implementation. It usually involves helping the staff to improve the service experience. Staff members act different scenarios when they come into contact with the users. They can also switch roles in order to gain deeper insights. It is used to understand how users are interacting with several touchpoints and to build empathy with the users. (TISDT)
In our case we used this as a discovery tool to find deeper insights in the doctors area. We did a service reverse role play where the patients and doctors switched roles. Here are a few videos that demonstrate that, followed by our key learnings.
Key Learnings:
- ● They felt good becoming doctors.
- ● The are was very open.
- ● Privacy is the main issue.
- ● Need for proper tourch.
- ● Need for popsicle stick when patients open their mouth.
- ● They should have a weight machine.
- ● They should have a blood pressure operator.
- ● Felt good that his medicine was changed on his request.
- ● Felt good when they when the patient welcomed them and said Hi.
- ● Felt like the patient was a friend.
- ● The surrounding made them uncomfortable.
- ● There was no privacy.
- ● There was a lot of rush.
- ● Lots of noises.
- ● Did not want to talk about their personal matters.
- ● She asked their problems with a smile on their face.
- ● She wrote and described the medicines prescribed.
- ● He felt shy.
- ● The space was congested.
Limitations: Actors may be shy and not be comfortable with acting. Acting a scenario may not be very close to the actual service.
Service Safari
A service safari is when people are asked to go out “into the wild” and explore what they believe is a good and bad service. Service safaris help you put yourself in the shoes of they user to understand their needs and encounters.
In our situation we asked the staff members to go out and experience any service, and then come back and have a group discussion on what was good about the service and what was bad. We then compared it to our service to see how we can improve or adopt certain features which would improve our service. We wanted to also compare our services to others.
The staff members explored, the Passport Office, Usman Institute (Educational Center), Zahid Nihari Restaraunt Bus Service, and Emirates Airlines.
I will now discuss the negative points and positive points of the service safari and how it related to our service.
Passport office:
- Agents were available outside to help you through the process.
- A text message is received once your passport is ready.
- There is a rolling token number on each counter.
- No signage.
- No flow chart or standard operating procedure.
- Only one camera to take passport photo.
- Need for more finger printing stations.
- No Reception.
Our thalassemia center does not even have proper signage. We learnt that not having proper signs makes the user uncomfortable and disoriented. We should set up signs around our center. From the one counter we learnt that we only have one doctor. We should have a female doctor. We should incorporate an SMS system to notify patients about closure of center, emergencies, token and appointment details. We should have a separate counter at reception for Thalassemia patients.
Usman Institute
- Head of the departments were involved with feedback for students.
- There was no smoking area. People were smoking at the canteen.
We should have our managing trustees involved in our feedback sessions. There should be a designated smoking area at our center.
Zahir Nihari Restaurant
- Food is good.
- The waiter comes right away.
- Food is on time.
- Billing takes a long time.
Our blood provides clean screened blood. There should be a bell system to call the staff members. Our staff should be more trained, have status reports for where the blood is in its own journey and an alert system which would be integrated into our software.
Bus Service
- Cost is low.
- Problem crossing the road.
- The bus is full sometimes.
- Does not stop in time.
- Does not wait for people to get off properly.
- Sometimes you need to run for the bus.
- No stopping system in the bus.
- Sometimes the bus does not come because of political strikes and gas price rises.
Road crossing problem can relate to our flow problem at the center. It came to our knowledge that our receptionist is always racing with answers without listening to the patients questions clearly. She should listen actively, think and then answer. We should have pick and drop services for our patients and staff at times of turmoil in the city.
Emirates Airlines
- Good problem solving attitude.
- Staff is good.
- In house services are good.
- Staff listens and cooperates.
- Fast track.
- Sometimes you have to wait a long time for the attendant. They often forget your order.
- Food choice is limited.
We should have more in house services.Counselling and guidance for patients and families. Staff should have a problem solving attitude. There should be a procedure for each task.
Feedback
‘I liked learning from other services and understanding cues” –Doctor
“Implimenting other services in ours would be beneficial. It is nice to hear other views good or bad. If others can do well so can we” -Nurse
A general comment after most group discussions is that this meeting should have been done earlier. Its good to learn from others and these exercises should continue.

Staff members discussing what the learnt at the Service Safari.
Limitations: Different people have different experiences.
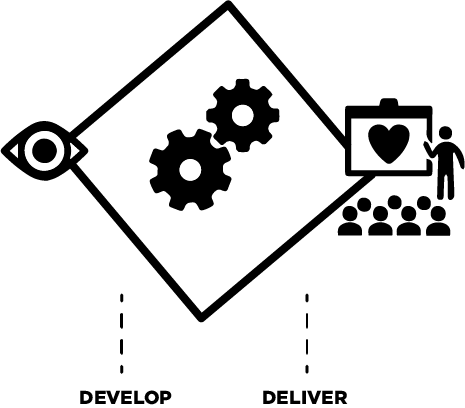
Idea generation
“Ideation is the creative process of generating, developing, and communicating new ideas, where an idea is understood as a basic element of thought that can be either visual, concrete, or abstract.” Gänshirt. (Gänshirt, 2007).
These techniques are in place to structure and inspire group brainstorming sessions(Stickdorn and Schneider, 2011).
We ideated around aspects of the service that had problems and room for opportunity. Some were specific while others were broad. Most ideation happened during our group discussions as we presented our insights and problems. It was almost natural for people to shoot out ideas when a problem was discussed. After our discovery and define phase we did have structured brainstorming sessions. As no one was familiar to other ideation techniques we kept it simple by just brainstorming around a white board and building on each others ideas.
We came up with several ideas which I will present in the following sections of service prototypes, what if, design scenarios, service staging, and desktop walkthroughs.
Here are a few photographs of our sessions:

Saqib provided us with a white board. We put it together at the center.

We were brainstorming around what would make the patients happy. A father knew his child really well and gave us some ideas.

A patient asking another patient to write some ideas so he could go paste it on the white board.
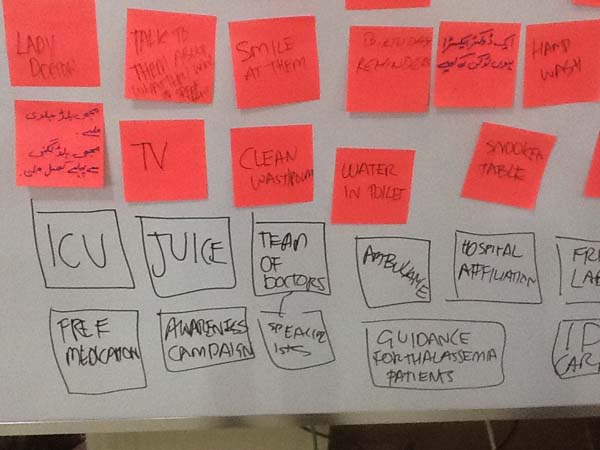

Brainstorming around how to improve the token system.

It was nice to have the white board on wheels. We moved it around the space to involve the patients. They could not gather around the board as they were being transfused.
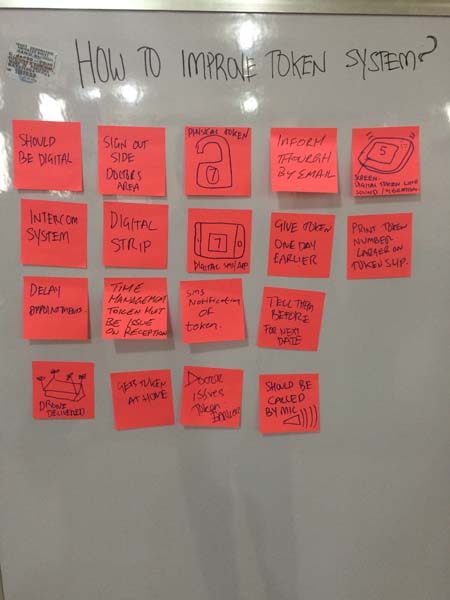
Results on how to improve the token system. We went decided to prototype the physical token and have digital displays.
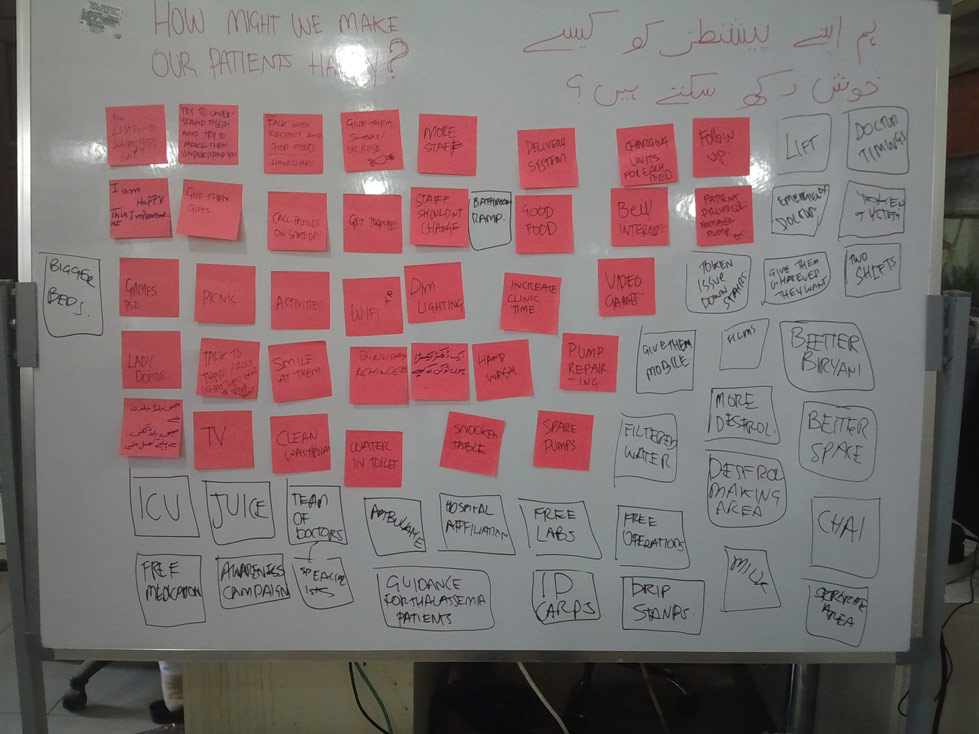
Results from how might we make our patients happy? We eventually ran out of post its and had to write directly with the board marker
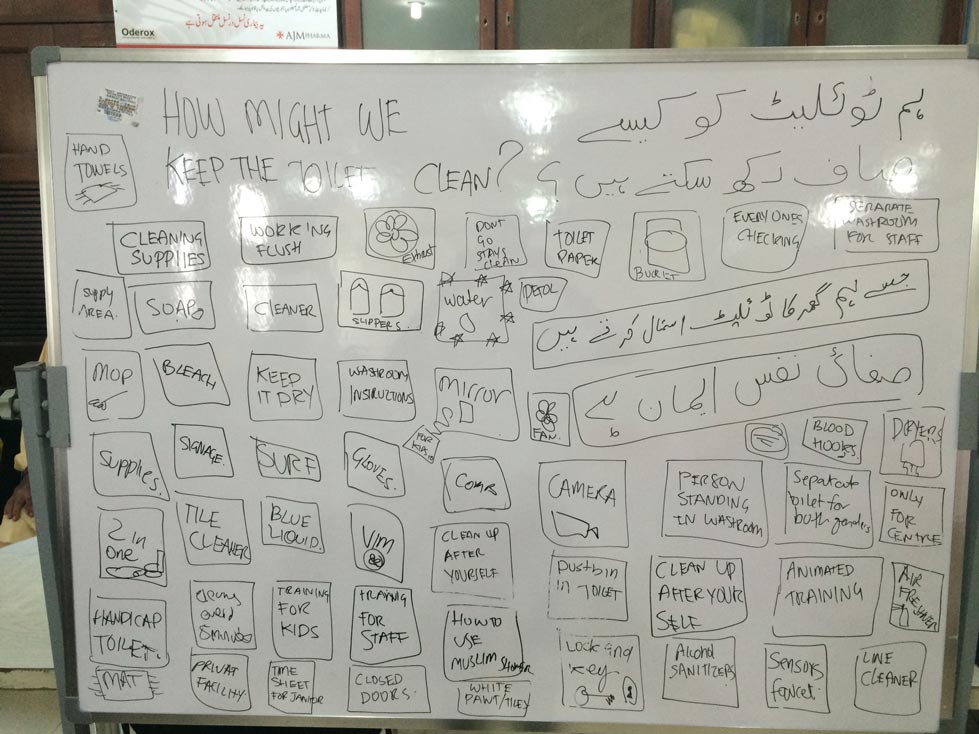
Great insights on how to keep the toilets cleaned. The patients realized that it is a shared between them and the staff of keeping the bath rooms clean as well.
Service Prototypes
“A service prototype is a simulation of a service experience.”- Marc Stickdorn (Stickdorn and Schneider, 2011) By prototyping you can save the organization money and time by designing and testing the experience before investing in technology to run the service. It is also very important to test the real people in the during development. It is important to make the prototype tangible as it will allow the user to experience it before hand. It also helps in getting feedback in what works and does not work.(Polaine, Løvlie and Reason, 2013).
Four levels of prototyping:
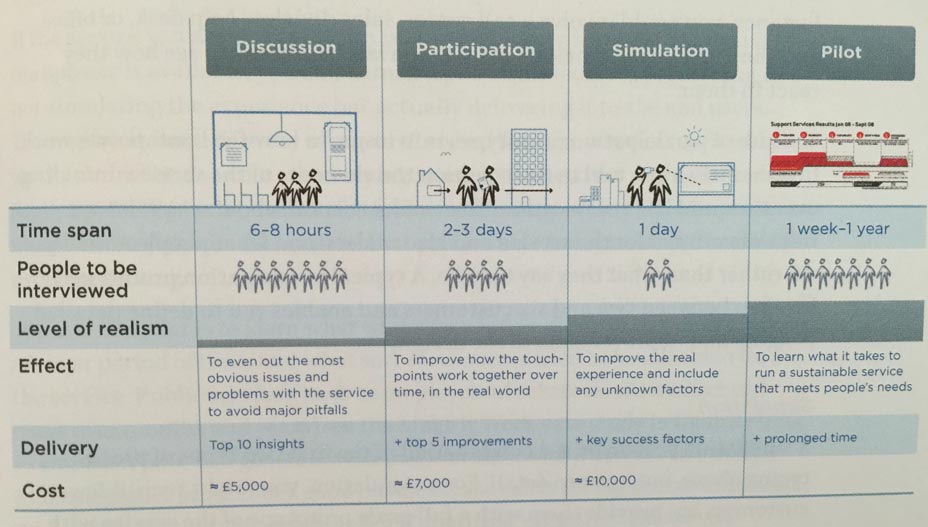
The figure about charts out the levels of prototyping. (Polaine, Løvlie and Reason, 2013)
The authors say that prototypes can range from quick solutions to elaborate stagings over longer periods of time. The four levels are as follows.
Discussion: Is a prototype in an interview style, where people choose different roles to react to different touchpoints of the service and provide feedback.
Participation: It takes place in the environment of the service, where the users interact with physical artifacts and the service provider is present.
Simulation: It is a combination of the first two but in more detail. It is usually a full scale prototype with more finished looking touch points. It can be done over a day or a couple of weeks to see how the user experience develops.
Pilot: This is providing the prototype to end user. It is almost finished and from this you can learn what works and does not work. A pilot is a beta service and has to allow room for an iterative improvement over a period of time and new approaches to problem solving.
(Polaine, Løvlie and Reason, 2013)
A prototype can also be as simple as a drawing.
Blood Delivery
From shadowing, interviewing and storytelling with the Office Assistant/Runner it came to our knowledge that it is difficult for him to go up and down the stairs multiple times a day. With the help of the maintenance department we came up with a prototype to deliver blood from the first floor to the second door via the back entrance. The runner from the first floor loads it and tells the runner on the second floor to pull it up. We made two iterations and made it under $5. You can see how it works from these videos.
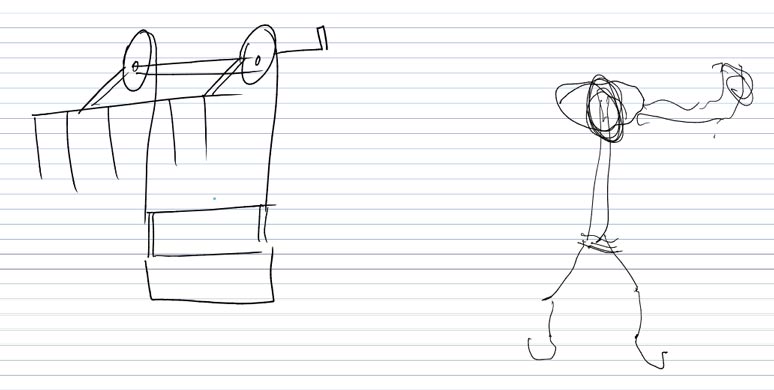
Drawing of transportation device before actually making it physically.
We tied a rope to the box which delivered the bag. The limitation of this was that the knots could open. We also thought that the spinning of the box could be a problem for the blood. But when we asked the doctor he said that it was not a problem. He actually said it is a good practise to shake the blood before transfusing the patient.
The was a second iteration of the delivery system With the hooks it is now more stable and easier to transport.
Results:
- ● Time is saved by 15-20 mins in the day.
- ● The runner is not always required to pull the blood up. Anyone can do it.
- ● The runner is no longer required to go up and down the stairs. He does not get tired and can focus his energy on different aspects of the service.
Another insight that we had was that the lab technician always has to find the runner downstairs in order to deliver the blood to the hooks. She has difficulty finding him. A solution we came up for this was to provide the runner downstairs with a wireless telephone and an extension number. So the flow would be that the Lab technician calls the Runner to deliver the blood. The runner places the box on the hooks and calls the other Office Assistant/Runner from his phone to pull the bags up.
To take this one step further it would be helpful to set up a service elevator or a pulley so not that much physical power would be needed for this task. Both costs are being estimated and the management will make a decision.
Husaini is building a new medical center where the Thalassemia Center is shifting. We have suggested setting up and a service elevator or a vacuum capsule system that could transfer larger containers from one area to another.
Bag Slip
From shadowing and interviews we realized that two same jobs were being done at two separate places. The lab technician would sort the slips with the bags and then send them separately to the second floor. Then the nurse would do the same thing. Lots of time was wasted in repeating this task. We brought this to the knowledge of the lab technician and the next day she sent the slips with the bag together.
From this video you can see how much easier this task is for her. You can also see how happy she is during this experience.
One of our insights were that sometimes slips get misplaced or mismatched. Attaching it with a zip tie helped solve this problem. We soon came to realize that it was a waste if you were using 50 zip ties a day. Reusable zip ties were not available in the market so we found a neat trick that if you put the string in the zip tie the opposite way you can pull it out again and reuse it.
The nurse finding it easier to double check this slips.
It is much easier for the nurse to take the bags out of the box. Slips will not get lost due to the wind from the fans either.
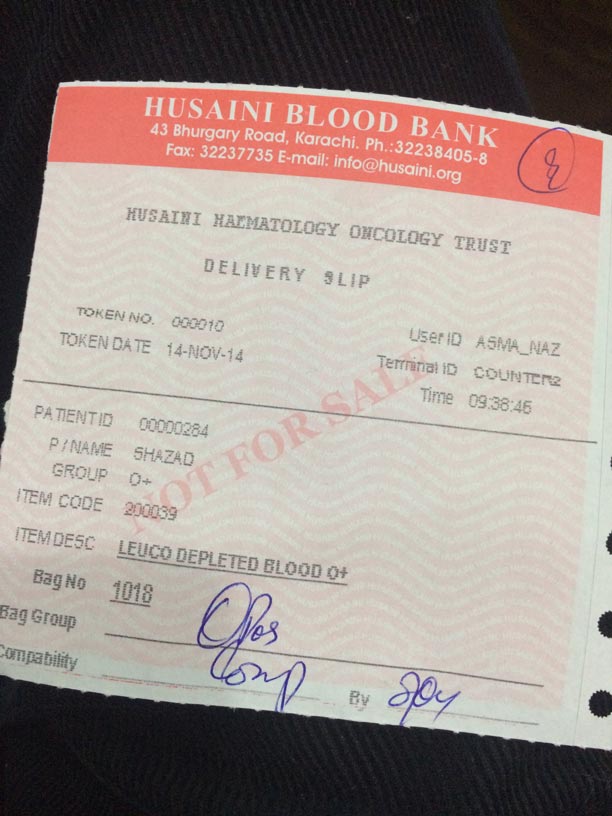
The nurse said that the token no. on the slip was small and hard to read.
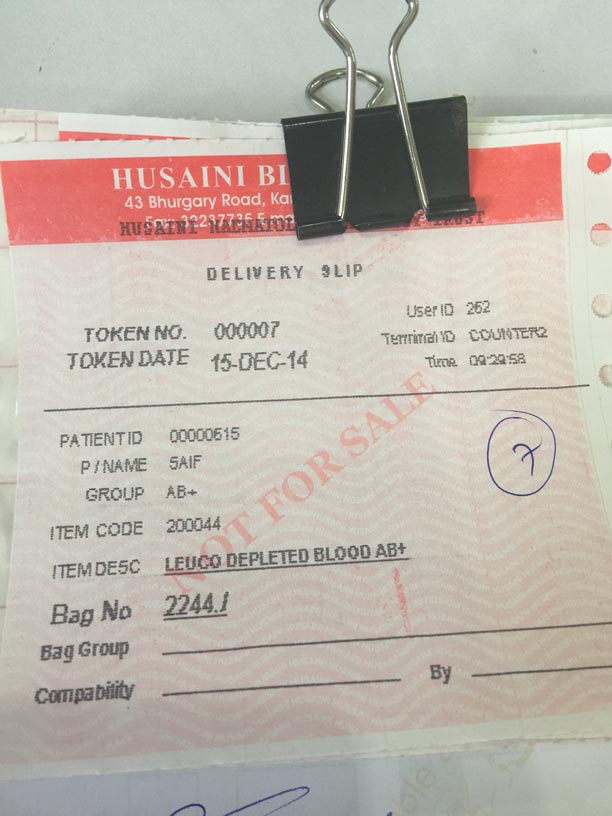
With the help of the IT department with asked them to change the code in the software to make the token no. bigger. It was much easier to read now.
Results:
- ● Time was saved by 15-20 min during the day.
- ● Easy to cross match slips
- ● Slips do not get lots
- ● Font increased so easier to see.
- ● Two jobs are not being repeated.
- ● Less room for error.
Future recommendations:
All our bags should have digital barcodes or RFID tags. This will allow for a smoother process. Also allow room for data collection. Less room for error.
From one of our insights that we had was that the donor never had any interactions with the patient.
If we make bar codes for digital data entry We can also make stories as we can know which person donated this bag of blood and connect them to the person they helped for marketing and awareness campaigns.
Physical Token
After speaking with the patients and shadowing the staff we realized that token that was issued to the patients often was misplaced as it was piece paper. We also saw that the nurse had to go around the room looking for patients by their names and it was disturbing them, and took a long time. After our brainstorm session on how to improve the token system we decided to make a physical token that the patient could hang on the blood stands.. The images and videos below will show the process and results.

First iteration of the physical token

Second iteration.

Nurse checking to see if he can see the token from the back of the room.

Testing them at the reception.
Nurse locating patients much more easily.
Results:
- ● Physical tokens helped for identification
- ● The Receptionist saved 5-10 mins as they did not have to physically write the token number and it was easier to give Hemophilia patients tokens as well.
- ● Nurse Staff saved 30 mins in the day as distribution of blood was faster,smoother and done silently.
- ● Patients were not disturbed by calling out of names.
Recommendations:
- From the feedback from the patients some said it would be nicer if it was smaller.
- Over time the prototypes are deteriorating. Need to make a final product in order for it to be sustainable.
Co creation with a patient. He recommended that we make it a heart shape to represent hope, love and to make it more friendly.

Patient showing his prototype.
Patient acting how he would put the token on the hanger.

Creation of the tokens.

Pilot launched. Hanging tokens still being used till today.

Patient hanging the token in an interesting way before he gets to his bed.
Digital Token System
We had several insights before creating this prototype. We knew that many patients would come to the second floor without their turn. Patients could not hear the call of the Office Assistant/Runner. There was no indication of which range of patients were upstairs with the doctor. There was a lot of rush on the floor. There was no systematic order or flow. Patients would often cut the cue. For this prototype we installed a mic and speaker for the runners voice to be head. We set up digital displays on both floors for the patients to know which token number was running. Here are a few pictures and videos of our process.

Set up a speaker on the bottom floor near the stairs.

Drew a range of token numbers on the iPad using Adobe Ideas to prototype a digital display.
Testing a digital display on the top floor with the doctor with a Wacom Cintiq Companion Hybrid. (Android Table) We put a slide show on the app Papyrus. We learnt that it was difficult for him to change the numbers from there.

First day testing the display. We set it up on a camera tripod. We learnt that not all patients could see the display.
Prototype being used during service hours to demonstrate how it works.

Mic set up on the top floor for the runner near the examiners desk.

Testing options of where the display could be set up.
2nd Iteration of the display for the doctor. The doctor can now swipe up using the Adobe Reader app.

Patient sitting with with doctor. Display visible to all patients in the waiting area.

Testing of controlling multiple displays via one device. We set up desktop screen sharing with two iPads via the Airdisplay app.

When we realized that patients could not see one display we set up two, one for each side.

A volunteer on the right side controlling the screen via a Macbook.
Results:
- ● Flow of the entire center was maintained.
- ● There was less rush upstairs.
- ● There was less noise upstairs.
- ● Seats were available downstairs
- ● Patients knew when to go up and when not to as they could hear and see the token numbers.
- ● Runner doesn’t need to shout and go downstairs.
- ● Doctor Saved 15-20 mins
Feedback and Recommendations:
- ●”The token system should be automatic and integrated into the software.”-Doctor
- ● It should be in Urdu and English.
- ● A digital voice or beeping system.
- ● There should be a display at the examiners counter as well.
- ● Digital integrated systems may give us data for time and flow management to continue to improve the service.
- ● “Its good to see that changes are coming”-Patient
Service Staging
“Service staging is the physical acting out of scenarios and prototypes by design teams, staff, or even customers in a situation”- Stickdorn Marc
We used this tool to explore the doctors space and what would happen if we were to set up a room. We used it to understand the flow of the patients in, around and out of the service. We also used it to demonstrate how our prototypes would work. Here are a few videos we captured of the floor manager. He often would act out situations. I had to explain that it is a powerful tool that could be used, and made him more aware that he was doing it so he could realize how it helped the process.
Floor manager exploring options if we had two doors for the doctors room.
Floor manager acting how the machine should be in order to understand the flow of the patient from station to station.
Feedback from Floor Manager.
- ● Its easy to convey your message.
- ● Easy to demonstrate how the service can be.
- ● It attracts the audience to come in and listen and give suggestions.
- ● Helps in developing consensus.
- ● Taking many suggestions to make the best decision.
- ● Helps sell the idea.
- ● It involves lots of participants.
Floor manager acting with the doctor to see if a room was set up how would the patients come in, through which door and where they would sit.
Floor manager acting as if he was using a prototype of a movable station for the nurses. He talks about how it can used for emergencies, draw for storing supplies and medical equipment, and trashcan at the bottom for disposal of used blood bags.
Desktop walkthrough
A desktop walkthrough is represented by a 3d model of the area where the service is taking place. Using simple props you can bring situations to life and help build prototypes. It allows for an iterative process of displaying many situations of the service.(Stickdorn and Schneider, 2011).
We used this tool to understand the space we were operating. We wanted to see if we moved around furniture or props to see how the flow of the center could improve.

Working together with a volunteer to put a 3D model of the building together using paper and cardboard.

Doing the Desktop walk through at the center helped us visualize the changes in real time. It was a co creative process between the Floor Manager, the Maintenance Department, Service Designer and the Doctor who is also the Head of the Department.

The floor manager explaining the flow if pieces were moved around. We also used a white board to right down ideas and understand flows.

Final result of how we thought the ideal use of space.
We decided to move around the furniture after doing this exercise.

The camp desk was removed and we set up the examination desk in the corner

We rotated the office assistant’s desk 90 degrees.
Results of the Desktop Walkthrough:
- ●We learnt that we could create a new desk for examination.
- ●The floor manager and assistants desk could be rotate 90 degrees to maintain flow in and out of the bed area.
- ●It also created space for Desfrol preparation and blood sorting.
- ●We could make a glass room for the doctor.
- ●Helped us plan a better ICU.
Results of Moving the furniture:
Doctor said:
- ● Better space for the height and weight machine. Its less congested.
- ● Open space for computer and data entry.
- ● Less disturbance.
- ● Less noise pollution because many people are not near the examination area.
- ● Open space made me feel good.
Nurse said:
- ● She felt good.
- ● There was less disturbance.
- ● It was more space to work.
- ● Attendees did not bother me as much.
Runner/Office Assistant said:
- ● Easier to keep track of the patients.
- ● Flow was much better.
- ● It was easier to handle the patients who would come for regular check ups and not transfusions.
- ● More space for the patients to sit.
- ● Doctor can observe the nurse.
Janitor said:
- ● The open space allows it to be cleaned easier.
Feedback on tool.
- ● It helped us utilize space.
- ● Easy to map and explain.
- ● Good to see it open from the top.
- ● Helps in planning and organization.
- ● Sometimes thoughts do not materialize physically. This exercise helped in that.
- ● Maximization of minimum space.
- ● Helps us understand what is feasible.
- ● It could be done on a 3D software but not everyone can use it and it is not as collaborative.
What if
“What if …” is a question that service designers may pose in order to prompt exploration of even the most outlandish scenarios.” -Stickdorn Marc.
It is used to explore wide-ranging changes rather than looking at specific touchpoints of a service. (Stickdorn and Schneider, 2011)
I had the pleasure of visiting Hyper Island in Singapore to brainstorm and bounce some ideas of some Hyper students. I had a very interesting discussion with one of the current students their. My supervisior Jerel had asked me to speak with him over the internet but somehow we managed to meet in person.
We brainstormed around the idea Can a Thalassemia Patient perform self transfusions. We thought around many ideas such as having a 24 hour service center where you can go and get blood and transfuse yourself. Many services such as banks, gas stations and restaurants have self service options. We wondered if the same could be applied at the thalassemia center. The self service machine would prick him for a blood sample, cross match it automatically and dispense a bag of blood with the transfusion kit and additional medicines if required. The machine would have a screen as well for guidance on how the procedure of self transfusion would be. If this idea could work it could possibly transform the entire system of how transfusions could take place in health care.
I was super excited about the idea and ran it past the doctors at the Thalassemia center. They said it would not work as the Patient will have difficulty pricking themselves and finding the vein. They also need to be monitored by the doctor and nurses during the transfusion, incase of emergency or an allergic reaction.
Even though this idea could not come to life yet. Who knows in the future what machines can do. Our moon shot thinking did not go to vain. It opened this idea of having a 24 hour service or home care which I will discuss in the Design Scenario section.
Reflection
This exercise taught me in order to improve health care services it is very important to get proper medical advice. Having moonshot thinking is great as we can always work backwards from an impossible idea.

Design Scenario
A design scenario is a hypothetical story with certain levels of detail in order to explore certain aspects of a service. They can be presented visually, acted out or simple text. They help create discussions how users will experience new aspects of a service in the future.(Stickdorn and Schneider, 2011)
In our case we thought of two possible scenarios. One where we would have a 24 Hour service and the other of delivery at blood at home. After running it by the management we realised that it is quite a premium service and would not be feasible for the organization at this point. It is something that can be considered when the new building facility is established. It would increase costs of running the facility(electricity etc) and additional salaries for staff members. It could be possible if the patient was willing to pay for it. As currently the blood bank does have a service where you can recieve blood tests at home if you pay for it. Some how it could get integrated into the blood bank.
Business model canvas
“The Business Model Canvas, is a strategic management and entrepreneurial tool. It allows you to describe, design, challenge, invent, and pivot your business model.” -Strategyzer.
Its a tool that brings clarity to an organization about its main aims while identifying its strengths and weeknesses.
We looked it as a tool to evaluate our current service, and see where there was room for improvement. We did three rounds of iteration on the canvas finding information that did not exist before. Here is our result below.

Sitting with the CFO and jotting out different segments of the Business Model Canvas.

Discussing new value propositions with the CEO
Feedback
CFO’s feedback. He mentions, it helps in documenting the system, it would help to get web contents clearly. Promotionals can be designed meaningfully. This will provide a holistic view of the activies that the activities they are involved in. How are they delivering the perceived services and what is the benefit of the receipt ant
CEO’s Feedback: He mentions it will help to enhance our over all operations because we are tapping each and every segment of our organization which starts from our blood donors who are the main suppliers of our blood. Our process starts from the blood donors till the patients who are on the receiving end. Whatever operations are between we are touching each and everything and this program(Business Model canvas) will definitely help.
Additional Learnings and Ideas:
From this exercise we also learnt that there is a need for a feedback system for both the staff members and patients. We also learnt that lately the company had not been doing any programs on awareness or prevention campaigns from Thalassemia. From my visit to the Thalassemia Federation of Pakistan Conference I learnt that most organizations were investing 40% of their budget on prevention programs. I also learnt that one of the centers was providing training to the patients to learn skills such as computers and crafts.
An idea popped into my head and I discussed it with the CEO to add to our value proposition and create a revenue stream as well. An insight that I had that most of our patients did not have jobs and were no longer in school due to their illness. If we were to provide training in skills to our patients we can engage them in prevention and awareness programs. They can also learn handicraft skills. With the goods they produce we can brand them in a way to help Thalassemia Patients in creating jobs, promoting awareness and spreading prevention programs. When this idea was pitched to the entire management in the final presentation, they took it very seriously and said they would plan to do something towards prevention programs.
Implementation
This section will cover the solutions our team came up with and presented to the managing trustees and board members of the Thalassemia Centre. We covered our process and presented our prototypes. I will take you through a list of solutions and recommendations. Several solutions were implemented during our design process as they were large concerns and needed to be addressed right way.
- ●Developing website for information, news, awareness, prevention, patient profiles, interactive map for way finding. Appointment management system based on requests for change and new appointments.(Approved)
- ●Sms notification system for patients.(Approved for testing)
- ●Pick and drop service. (Request pending)
- ●Separate counter at Reception for Thalassemia Patients.(Request pending)
- ●Tokens will be issued downstairs if patient comes without appointment. Doctor will give approval over the phone so the patient does not need to come upstairs to get slip signed. This will maintain the flow and would not cause disturbance to the doctor and other patients. (Approved)
- ●Tv in waiting area on first floor.(Request pending)
- ●Designated waiting area for Thalassemia Patients. Attendees will receive a wrist band for priority seating. (Approved, testing results)
- ●Signage to be installed around the center.(Approved)
- ●Mic is being used from the blood bank to call patients now. (Implemented)
- ●Digital Token Displays (Approved, implementation is happening next week with integration with the software to get data on time taken between each touchpoint and how long long each touchpoint and patient takes with the doctor)
- ●Curtain for Examination area (Approved)
- ●ICU curtain (Approved)
- ●Extra nurse staff (Request Pending)
- ●Furniture movement (Approved)
- ●Removal of Camp Department Desk and Stuff(Approved)
- ●New Tvs (Approved) one new Tv installed.
- ●New longer beds (Approved for new building current location does not support the space.)
- ●New Air Condition (Approved, implementation very soon already in the pipeline.)
- ●Movable station for staff member (Request pending)
- ●New Stands (Approved , in the implementation pipeline)
- ●The solution we came up for the food is to request other restaurants to provide us with food a couple of times a month. We would share their compassion over our social networks. It would be CSR for them as well as marketting.
- ●Set up of candy jar for the patients (Approved)
- ●Hand sanitizer stations( Request pending)
- ●Sitting are for staff (Request pending)
- ●Medicine preparation area for Office Assistant (Implemented)
- ●Uniforms for staff members (Approved)
- ●ID cards for patients (Approved, Data collection for implementation starting in January)
- ●Telephone for runner (Approved)
- ●Reusable Zip Ties (Approved and ordered Internationally)
- ●Oxygen machine for ICU (Request pending)
- ●Games and better entertainment for children (Approved)
- ●Picnics and outings for patients(Request Pending)
- ●Lift system for blood (Request getting investigated for costs and feasibility)
- ●The Runner is very happy with the current prototype for blood delivery. It is continued to be used till today
- ●Physical token needs to be made into a final product (Approved)
- ●When we say free service we should be able to provide our patients with everything, from medicine to diagnostic. (Request under investigation)
- ●Full dose of Desfrol for iron chelation. (Request under investigation)
- ●Counseling and Psychotherapy for patients. (Request pending)
- ●Other specialized doctors for other problems. (Request under investigation)
- ●Awareness and prevention programs. (Approved)
- ●Donation drives. (Approved)
- ●Employment opportunities. (Request pending)
- ●Skill development for patients.(Request pending)
- ●Separate timings for Bank al Habib patients.( Request under investigation)
- ●Possibility of 2 shifts. (Request may be possible in new medical facility)
- ●Role management system. (Request pending)
- ●CLEAN DRINKING WATER. (Approved)
- ●Wifi, Electric outlets for pump charging (Approved)
- ●Hooks for blood bags in toilet. (Implemented)
- ●Sitting area for staff. Balcony can be converted for mini pantry. (Request denied as a new AC unit is being set up in that space)
- ●Call button for help. (Request pending)
- ●Headphones for patients(Request pending)
- ●Integrated ramp on stairs for wheelchair(Request pending)
- ●Lift (Approved for new building)
- ●Integrated technology system for patient history, medicine dose, examination.( Approved, implimentations happening in new software)
- ●Better software. (Approved, currently being developed)
- ●Better communication amongst team members.
- ●Instruction manual and illustrated SOPs(Request pending)
Below are a few images which have been implemented.
- Better Measurement tools (Implemented) We received a two in one weighing machine and height scale. We also got a digital weighing machine for babies.

- Doctors testing new machine.
- Separate doctors room (Implemented)

- Patient sitting with doctor. Both patient and doctor was very happy. We are just waiting for the curtain blinds to be set up for more privacy of the room.

Lady Doctor Hired.

- Patient has a Desfrol making area now, after we moved the space around.

- New LCD Tv set up. Patients were thrilled. Staff also was not afraid of the Tv falling on her head.
- Bathrooms cleaned and a janitor hired to primarily clean the toilets. Locks were also installed on the toilets and patients could not use it without getting the keys. This would the bathroom cleaner and gave them a sense of responsibility as they had to return the key and present the bathroom the way they got it. Time sheet set up for janitor. Janitor was responsible to clean the washroom after every use. New cleaning supplies were provided to the janitor and he can request for any additional supplies he needs whenever he wants.
-

- Clean washroom with running water.

- Muslim showers installed and bathroom much cleaner.

- New soap dispenser installed.

- Stairs Painted.

- Had a meeting with all the janitorial members. Came up with several solutions to keep the place clean. Some have been implemented some have not. The management needs to to continue to follow up.
It is very important for this conversation to continue. There is a need for weekly internal center meetings and a meeting atleast once a month with the top level management. The trustees need to be more involved. Everyone should know their roles and take responsibility for it. There needs to be active communication A platform for feedback for staff and patients to continue to make our center better. These tools that have been introduced should be practiced to gain further insights and come up with ideas and solutions for problems of the future. This practice should also be done with other departments so we can see HHOT as an entire holistic system working as a whole rather than separate divisions.
Feedback
Service design is an on going process. We may start somewhere but we will continue to iterate through re-discovering and re-creating the service experience. I would like to present the feedback I received at the end of the period of my Advance Work based project after I presented it to the Board of Directors, Managing Trustees and Staff Members.

Receiving feedback after the presentation.
“There is lots of improvement, but mainly it is clean now!” –Patient
“The doctor’s office is good, there is less noise, everything is more relaxed, we can have privacy, the hanging token helped us book our bed so no one would take it.” –Patient
The rush is less. We go in one at a time now. Everything goes according to their own turn now. No one is cutting the line. I am happy and it is more stylish.” –Patient
First the bathrooms stank now they smell good.” –Patient
Everything is running on time now. Food is better, the washroom is better. Everything is visible now. Hopefully the center will continue to improve.”-Patient
“Mr. Hasan Habib through his vision and wisdom highlighted some of our mismanaged minor & critical operations. After discussion and approval from the HHOT management he made necessary changes which ultimately resolved almost all our operational issues and lead to the smooth functioning of our center. We found him creative, dynamic, dedicated and result giving. I wish him ever success in his future life.” –Dr Saeed Ahmed (Consultant & Head Blood Bank, Thalassaemia & Hemophilia Center)
“It is stated that you did wonderful job regarding Thalassaemia Project in Husaini Thalassaemia care center. You were practically involved in all the procedures regarding thalassaemia and indicated very well the weak points of organization and also present the solution of problems. I appreciate your hard work and dedication towards you aim but there is still room for improvements regarding betterment of patients of Thalassaemia. Regular visits of consultants like General Physician,Cardiologist,Endocrinologist at center to rule out the systemic complication produced due to Blood Transfusion. An excellent intensive care units with Adult and Pediatric ventilator support. 24 hours fully loaded ambulance for any acute emergency and many more concerns which are not impossible to solve by a man like you.” – Dr Agha Umer Draz Khan ( Consultant Pathologist, Husaini Blood Bank).
“Thanks for taking out your time to conduct the activity of “Service Design Thinking & Process” for Husaini. The activity is highly appreciable because it addressed the complete flow of our work in detail, even minute operations were also taken in account. The problems were highlighted and appropriate solutions were suggested. The exercise will definitely be helpful to bring innovations in the operations to improve quality of services for the patients and ease of work for the staff members in a very simple and practical manner. The beauty of the process is, it was a total participative exercise as far as staff and patients (customers) are concerned which is very important for the successful implementation.” – Asad Ali (CEO)
“It was a pleasure working with you. Your assignment was a very useful activity for us, here we would like you to request that you please spare same more time and do the same exercise for rest of our divisions to help improve our service delivery.
Few tools and techniques you used were certainly very useful and Interesting learning for us,
- Business Canvas Model
- Customer Journey Map
- Service Blueprints
- Storyboards
- Contextual Interviews
- Expectation Maps
- Design Scenarios
- Idea Generation
We will implement your recommendations and we thank you for your support to our charitable Trust. ” – Shaikh Zulfiqar Ali Hashmi (CFO)
“It felt good that someone came in and took an initiative to make a difference. In the past four years that I have been here no one has been involved. I liked the card sorting exercise as it hilighted the problems in order. It was nice that the white board was taken around the room so the patient could contribute directly to the brainstorm session. Change has come about after you came. All the bathroom problems are fixed. I like the token system, as the rush is maintained. It was nice to have the interviews as things were told from our hearts and the patients hearts. There should be a team of doctors or some doctors should come in sometimes a week. What could have been improved is to give a patients and staff a feedback card so they can write whatever the feel whenever they like.” Naimat Ali (Runner/Office Assistant)
“I liked the process. I wish you could have come earlier. I wish that this continues to say the way it is after you leave. From the washroom, token system to the doctors room it is great. The best is the blood delivery system as it helps helps the other other assistant. The food should also come up the same way. I liked the card sorting as it helped us identify which problems the patients were facing. We should have more meetings and someone to come in to do more of these processes. We liked the tools but it is difficult for us to take out time to do it ourselves. No one asked about us before you came. It was nice that you were involved in the process.” -Saba Zehra ( Office Assistant)
“You created an environment to allow people to say what’s on their mind and heart. It’s like an Art. When our multiple requests and complains were not taken into account before we felt that they did not have value. So we stopped talking about our problems. Some things may not be implemented but you are allowing them to think another way. Broaden their thought process. The desktop walk through helped us see something from the top. We tried the changes required and it was successful. Facilitated an area for people to voice their thoughts and suggestions. Involved the stakeholders to resolve the problem. It was good to involve more people in the process. Once a system is developed its nice to continue to keep it going, regardless if the stakeholders change.” Zeeshan Haider (Floor Manager)
“I like how the slips come up with the bag now, it has made my life easier. Also the new measurement tools allows for a more accurate reading. The interviews felt good because everyone could voice their opinions. The tools and methods helped as what was not working before is working now.” Naheed (Nurse)
It felt good to make changes for the patients. It was nice to ask the patients about every step. It was good to get the washrooms cleaned. The identification of an extra helper has definitely helped. Felt good to be interviewed and seeing every little aspect of the process. We listened to every little aspect of the problems and it feels good to see them getting addressed. Jutti Aunty (Janitory/Helper)
“Your attitude was good and talking to everyone on the same level. We understood how to understand on a deeper level and got the patients and employees to tell us what was in their hearts. The token system practise was good and the patient feedback was great. Some patients said we wish this system was put into place before. The room has helped in allowing the patients to talk openly and about their private concerns. Things were identified which were over looked before. Now we are promoting a clean hospital environment. The new type of thinking introduced us to new knowledge and showed improvement in patient experience.” -Dr Mushtaq
“Thank you for your presentation yesterday. We were very impressed with the way you conducted the study. You followed the methodology which you presented at the beginning of your talk properly and took us through the whole process. We were happy to see that you did a thorough investigation of the processes and that you were involved in every stage of it. This accounted for a very in depth study and the results prove that. We strongly feel that the suggestions which you have made is worth implementing . This will surely give us more efficiency and productivity. Your suggestion to hire a lady doctor is well noted and we would implement this as soon as possible. We were impressed the way you reshuffled the place ,it ddefinitely made a difference in the work flow. Your recommendation for making the ICU more private by installing partitions is also well noted. We will also implement the recommendations you made regarding the elevator and other means of transporting the blood bags . In the end we would like to say that you did this project with total hard work and dedication , as if you owned this institution. We are quite sure that if we had given this task to a Consulting Firm, they would have at least charged us Rupees 1.5 to 2.0 Million. Thank you again for doing this project ,our team at Husaini is indebted to you. Wish you all the best in your future endeavors .” – Murtaza Hussain. (Managing Trustee)
“You can clearly see the difference your team made.. It didn’t seem to me that they were doing it because they had to. They bought into the process. And you explained the tools in a very simple way. When you talk to them about stories, I’m sure you told them about why story telling is important. We are not a very service oriented company. So it is an approach which is very important. Like I told you today we are going to do it with the other eight departments. Just the fact that I am asking you to do it means that I am convinced by your process. You sold me. You are using the right process and the right tools. But most important is that you sold the process and concept to the team and it clearly shows. I want to go into great details about the problems you addressed. I want to sit with the team and go over it again. I saw the staff members during the presentation. There were no closed arms. They were engaged and that to me is success. Even somethings were like, if you look at the bigger picture, saving lives, saving time a couple of minutes here a couple of minutes there, its more about an attitude shift. We are growing and we need this. We have 80 outlets (Other divisions of HHOT). How do we see the type of service they are getting there? There needs to be processes and SOP’s. Everyone needs to be on the same page. We need to improve our communication and define our goals clearly. That will be the next thing, mission purpose of the organization. Again this is a start, we need to go over it again with you. It was good you gave them respect and you became part of the team. It was good and professional. You gave 3 months and it shows. It is a question of vision. This is a process, and about correct thinking. What you are doing right now, there is definitely going to be a demand for it in Pakistan!” – Munawar Rashid (Managing Trustee)
Conclusion
This advance work based project, was set out to explore how service design thinking would improve service provider and patients experience at a Thalassemia Center, and recommendations on how the center could continue to use the tools and methods in the future to continue innovating. The process revealed that using the tools and methods of service design thinking did improve over all experience at the center. This was measured by the feedback provided by the service providers, staff members and patients. The management team has agreed to hold more meetings to discuss current problems and set plans to implement the solutions that were suggested. Not until each touch point works as a part of the whole service will the users get a holistic experience.
As far as using the tools and methods in the future it is important that the senior management or an external service designer gets involved in order to facilitate the process. It has to be a team effort and the organization will need to take out time to go through the process again. Initially it was difficult to create the culture where the service providers and the patients were open about talking and presenting their concerns. Now that they are more open to discussion it is important for the management to keep continuing the conversation. Many patients and staff members said “what will happen after you leave and will there be more people like you coming in to do this process again.” That to me showed that they were engaged and open to the process. Secondly another thing that validates how they will continue this process in the future is that one of the managing trustees asked me to perform the same project for their other divisions. Lastly it is very important to make a tool kit or guide of service design thinking in the native Urdu language, in order for the organization to better comprehend the process. It was very challenging for me to translate the tools and methods on the go and there was a possibility of misinterpretation by the users who took part in the process.
As far as I know there are no service design agencies in Pakistan and, and this kind of project is first of its kind. I hope this project sets a foundation for people in my country to understand how the tools and methods were used and how they helped improve overall experience. I am curious to see how service design thinking will evolve in Pakistan and continue creating new experiences.
Journey
My journey as a designer began in Vancouver after I graduated with Honors from the Vancouver film school in Digital Design. My award winning project (rebranding of Husaini Blood Bank) got me a job as the Brand Manager for Husaini Blood Bank in 2012. I worked for them as a freelancer maintaining their brand identity and handling their social media platforms. The new identity was successful and between 2012-2014 their branches have increased from 20 to 80 with all storefronts and departments incorporating my designs. It was a very rewarding feeling as my designs were for social good.
Along side this I worked in creating children story books for the iPad with StoryPanda in Vancouver and then worked with e.d Films to create motion graphic films for educational purposes.
I had intentions of moving back to Pakistan as I had dreams of staring my own design agency and educating students about design. Due to the economical situation in Pakistan I knew that getting a job as a basic designer would not get me much income. I also wanted to grow as a designer, explore different fields of design, learn how to work with teams, manage projects and nurture my self to be a leader.
Working at my dream job in Montreal, still did not discourage me from applying to Hyper Island as I knew I needed to continue to grow as a designer. I got accepted and my Hyper journey began.
I had no idea what to expect. All I knew is that I had to go in with an open mind and be open to new ideas. “Learning by doing” was a concept I was really excited about. My work was always hands on and this was just another step to empower myself to become a better designer.
In way week we were introduced to many concepts such as the learning spiral, johari window, active listening, team building and feedback. These concepts set the tone and culture for the months to follow. It taught me to learn more about myself and others. These methods were practised as almost second nature throughout my time at Hyper and during my advance work based project.
Learnings from Hyper Island modules.
Design Thinking: I had designed, brands, websites, infographics, animations and many other creative things in the past. But never did I truly think about the design process.
The introduction to the double diamond was like opening my eyes and expanding my horizon. In the past I had mainly designed through gut feeling. With the double diamond method I learnt that it’s important to discover insights, define problems and opportunities, develop ideas and prototypes and deliver concepts. These were the same principals that set the foundation for my advance work based project.
Andy our mentor for Snook introduced us to service design. He had been working on projects that produce great outcomes for the community. It inspired me to get to know more about service design and immerse myself in this field.
Digital Technologies: I was familiar with coding in the past, but not about bridging the gap between tangible artifacts and digital technology. Being introduced to makey makeys, audrinos and raspberry pies opened up a whole new playing field for me. User Experience played a great role here as I understood how small tasks performed in a sequence created an experiences as a whole. Even as little as making a cookie jar that prompted that it should be refilled once the last cookie was removed taught me about if then that scenarios. It also taught me that difficult tasks can be achieved if you break down the steps.
This really helped me when it came to planning and understanding the tasks the patients at the Thalassemia centre had to perform at the service. Rapid Prototyping also played a great role as it taught me that we could make quick solutions, test if they worked or not, get feedback and then repeat the process.
Business Transformation: This module taught me how to understand value chains, business models and value propositions. Working with Belvita biscuits I learnt how to find opportunities on how to introduce business transforming ideas to a biscuit brand. We learnt about moon shot thinking and finding concrete evidence as to why a business should change. I think breakfast biscuits was a transformation in itself as who knew that one would have biscuits for breakfast.
Understanding business transformation was essential to my project. Working with the CFO and CEO with the business model canvas we identified new opportunities for creating new revenue streams for the organization. We even had some moonshot ideas such as having self service for blood transfusions. Some of these moonshot ideas would not work, but we learnt to cut back from a big idea as it would spark some insights elsewhere.
Start Up: Along with four other class mates we decided to create a service design agency. Our love for service design brought us together. Our brief was to brand a company and pitch why it was relevant to the current market. We took this one step further by actually making our services real and testing if we were hireable. We landed two clients and completed two briefs. One of the clients wanted to even hire us after we presented our concepts. In my opinion this was success.
This module taught me to follow my passion. After completing this last module I had to figure out what I needed to do for my Advance Work Based Project (AWBP). I wanted to explore something to do with service design in Pakistan. My initial approach to the project was bridge the gap between service design thinking in the west with how it was done in Pakistan. I began to search online to see if anyone was doing this sort of work in Pakistan and I could not find anything. I then began to speak with people in the creative industry to see if they knew of any. I spoke with someone from Ogilivy, The Brand Crew, Cre8tive Bench, and some ex-owners of JWT. One of the people I interviews had also worked for Digitas Lbi in USA a few years ago. I asked them about what Service Design meant to them and if anyone was practising it in Pakistan. Here are a few videos of the interviews.
The main learning I identified was that no one was practising service design in Pakistan, by its main core principles. Companies were enhancing customer experience but not necessarily taking a service design thinking approach. I wanted to introduce service design thinking to Pakistan but my supervisor told me that that was to broad. He said I should narrow my focus. He also reminded me that it has to be work based. I then thought why don’t I try service design thinking with an organization in Pakistan. He thought that was a good idea, and my starting point was there.
Since I had been working towards my first statement of bridging service design thinking between the west and Pakistan, I had set up two meetings in Manchester with service design agencies to understand how they worked and approached projects. Even though my focus had shifted I could still learn from them. My experience with the agency was quite insightful. They were in the development and deliver phase of their project. They had been working with a chain of hotels to see how they could improve their service. They allowed me to shadow as well as participate in their process. We had several ideation sessions, and prototyped on paper how the experience of a new website would be. My learnings from their process was that it was very important to have a proper schedule and process to each development task. Another thing that I noticed was that during the brainstorm sessions, the client and other stakeholders such as, end users, staff members and management team were not involved. So as far as a co-creative process is concerned I feel that there was room for improvement. With the second company I came in during a time where the agency were shifting locations. I did not get much time at all to understand their process. They involved me in one brainstorm session which was done over skype with one member of their team overseas. They were also developing a website to engage users to sign up for sports camps online. From that one session I learnt that the client and other stakeholders were not involved. Only three people were in the ideation session including myself. It was more of a conversation than idea generation. Team members were not building of each others ideas. The connection was poor so it was difficult understanding one another.
My learnings from visiting these agencies are:
- It is very important for the projects to be co-creative.
- Ideation should be done in context of the service.
- Ideation should be done in person.
- It is important to have structure when approaching a project.
- Feedback is essential for a better outcome.
I took these learnings and applied them to my project.
Initially I was looking at how to improve the services at Husaini Blood Bank, but I soon realised that there were very few returning customers, as people only donated blood when their family or friends required blood. The other users of the services were regular donors who would donate for social good. These users could only donate a maximum of three times a year. Due to the less frequency of these users interacting with the service it was very difficult to do a service design project given the time from of my AWBP. I raised my concerns with the management and they suggested that I could do the project with Husaini Thalassemia Center instead. This was more achievable as the patients would visit the center at least twice a month and I could work with them to improve the service.
The first step of my project was to do visit the center and understand how the service was delivered. As soon as I entered, I realised that there were no signs anywhere in the premises from the entrance to the washrooms. I already knew that there was opportunity. I then understood what thalassemia was and how the staff members were providing the service. I then held a meeting with the staff members and the management team to propose how might service design thinking improve the service they were offering.
After the first presentation the response was great and the staff members were very excited. The staff members had never been in a group before this time. The CEO as well as the janitor were in the same room. This made the janitors feel very good. Right after I presentation the staff members decided to have a group discussion on the approach of the project. They also started raising concerns and problems of the service that they experienced right away. The level of comfort was great. Due to the shortage of time we decided on a schedule of how to approach the project and which tools and methods will be used when. One of the largest challenges I faced was being able to communicate in my native language Urdu with the team members.
The approach we used was the Double Diamond. The discovery phase was very interesting. I soon realised that there were many operations that were happening behind the scenes that needed to be addressed. There were also many concerns from the patients side as far as cleanliness and privacy when visiting the doctors. I will not cover any more insights as they have been mentioned in the sections before. I will discuss my learnings about the process in particular. It was very important to have all stakeholders on the same page. It took two weeks before the staff members and patients were comfortable with the process. In the start they were not open to sharing insights which were in their hearts, but with time they were more comfortable. As soon as we discovered that the toilets needed attention, the issue was addressed right away. Within two days the toilets were cleaned and the broken utilities(muslim shower, flush, taps) were replaced. This happened during the discovery phase as it was a bare necessity. As the patients and staff members saw that the process was bringing about change they were more open to sharing their thoughts and involvement in the project. Before this staff members were afraid of losing their jobs and the patients feared that their free service would be revoked.
During the development phase the staff members were very cooperative. They even took out time after work hours to have group discussions and brainstorm sessions. Prototypes were made and tested at the location. The quick feedback helped us iterate the prototypes and allowed us to test multiple times. We had great results. We saved over an hour of work time once all prototypes were put into place. This helped the patients flow better throughout the premises, time spent during each task was reduced for the staff members as well as the patients and the blood delivery system helped the staff members from going up and down the stairs multiple times a day. We had one final group reflection on the entire process and made a proposal for the management on what changes were required in order to continue to improve the services.
Being part of the process from start to end helped me empathize with the patients as well as the staff members. Understanding what drove each stakeholder helped in the success of the project. The project resulted in a stronger team between the management and the staff members. It allowed for patients and staff members to voice their opinions. Many of the concerns were implemented and several others are in the pipeline. One of the managing trustees also wanted me to repeat the same process with their other divisions. This was a sign that shows me that it worked.
For me success was seeing that this process could bring positive change. It empowered the service providers as well as the end users.
As this process was done for an organization that provides free service I was very curious to know how open other organizations would be to the process which had paying customers. I presented my learning from this project to some people and the feedback was great. A few people want to invest in me opening a service design agency, and another person requested that I should see him to see how I could establish a department in his firm looking at customer experience and engagement. I am looking forward to seeing service design evolve in Pakistan.
Lastly I would like to thank everyone who was part of this project. Family and friends for support, Hyper Island for guidance and Husaini Hematology and Oncology Trust for being cooperative and part of the process without whom this project would not be successful.
References
+Acumen, (2014). Design Kit: The Course for Human-Centered Design – +Acumen. [online] Available at: http://plusacumen.org/courses/hcd-for-social-innovation/ [Accessed 21 Dec. 2014].
Affairs, A. (2014). Contextual Interview. [online] Usability.gov. Available at: http://www.usability.gov/how-to-and-tools/methods/contextual-interview.html [Accessed 18 Dec. 2014].
Alejandro, R. and Colin, L. (2012). A methodology for connecting User Centered Design (UCD) with Eco-design. The possibility of migration of products to services based on the user acceptance.
amity, (2014). What. [online] Available at: http://www.amityhcd.co/ [Accessed 1 Dec. 2014].
Brown, T. (2009). Transcript of “Designers — think big!”. [online] Ted.com. Available at: http://www.ted.com/talks/tim_brown_urges_designers_to_think_big/transcript?language=en#t-794611 [Accessed 23 Dec. 2014].
Brown, T. (2014). Design Thinking | Thoughts by Tim Brown. [online] Designthinking.ideo.com. Available at: http://designthinking.ideo.com [Accessed 23 Dec. 2014].
BSR, (2011). Stakeholder Mapping.
Businessmodelgeneration.com, (2014). Business Model Generation – BMC. [online] Available at: http://www.businessmodelgeneration.com/canvas/bmc [Accessed 20 Dec. 2014].
Cliver, M., Hegeman, J., Lee, K., Libert, L. and Tennant, K. (2007). Design for the Clinic Experience.
Daylight, (2014). What is Design Thinking. [online] Vimeo. Available at: https://vimeo.com/90355541 [Accessed 23 Dec. 2014].
Denning, P. (2013). Design thinking. Commun. ACM, 56(12), pp.29-31.
Design Council, (2014). Introducing Design Methods. [online] Design Council. Available at: http://www.designcouncil.org.uk/news-opinion/introducing-design-methods [Accessed 23 Dec. 2014].
Design Council, (n.d.). A study of the design process. [online] Available at: http://www.designcouncil.org.uk/sites/default/files/asset/document/ElevenLessons_Design_Council%20(2).pdf [Accessed 4 Dec. 2014].
Designkit.org, (2014). Design Kit. [online] Available at: http://www.designkit.org/methods/24 [Accessed 19 Dec. 2014].
Designkit.org, (2014). Design Kit. [online] Available at: http://www.designkit.org/case-studies/4 [Accessed 21 Dec. 2014].
Dictionary.com, (2014). the definition of experience. [online] Available at: http://dictionary.reference.com/browse/experience [Accessed 3 Dec. 2014].
Engine Group, (2011). Embedding community engagement. [online] Engine. Available at: http://enginegroup.co.uk/work/public-services-in-buckinghamshire [Accessed 23 Dec. 2014].
Engine Group, (2013). Tailoring services for Virgin’s customers. [online] Engine. Available at: http://enginegroup.co.uk/work/virgin-atlantic-heathrow-customer-experience [Accessed 5 Dec. 2014].
Gänshirt, C. (2007). Tools for Ideas. Basel: De Gruyter.
IDEO, I. (2011). Human-Centered Design Toolkit. 2nd ed. Authorhouse. pp. 6
Kaiser Permanente, (2012). (Re) Imagining the Care Experience.
Kelley, T. and Kelley, D. (2013). Creative confidence. New York: Crown Publishing Group, pp.19, 20.
Perrott, B. (2013). Including Customers in Health Service Design. Health Marketing Quarterly, 30(2), pp.114-127.
Polaine, A., Løvlie, L. and Reason, B. (2013). Service design. pp. 30,129-127,141-143
Steve Vargo., and Lusch, R. (2012). Toward a better understanding of the role of value in markets and marketing. Bingley, UK: Emerald Group Pub.
Stickdorn, M. and Schneider, J. (2011). This is service design thinking. Hoboken, N.J.: Wiley. pp. 23-25,32,38,82,115-127,143-209
Strategyzer, (2014). Business Model Generation – BMC. [online] Businessmodelgeneration.com. Available at: http://www.businessmodelgeneration.com/canvas/bmc [Accessed 6 Dec. 2014].
Tassi, R. (2009). Customer Journey Map | Service Design Tools. [online] Servicedesigntools.org. Available at: http://www.servicedesigntools.org/tools/8 [Accessed 17 Dec. 2014].
Thalassemia.ca, (2014). Disease & Treatment « Thalassemia. [online] Available at: http://www.thalassemia.ca/disease-treatment/ [Accessed 11 Dec. 2014].
Vianna, M., Vianna, Y., Adler, I., Lucena, B. and Russo, B. (2012). Design Thinking. Berlin: Logos Berlin. pp.13-14
Wales, N. (2014). Give Blood – FAQs. [online] Give Blood. Available at: http://www.blood.co.uk/giving-blood/faqs [Accessed 13 Dec. 2014].
Warner, B. and Simon, H. (1969). The Sciences of the Artificial. OR, 20(4), p.509.
Zuber, C. (2011). Infrastructure of Design.
Designed with love By RocknRolla